


CLINICAL CHALLENGES
The Case of the Botched Surgery?
When a cataract extraction doesn't resolve
a patient's problems, this doctor steps in.
![]() By Eric Schmidt, O.D.
By Eric Schmidt, O.D.
I first met C.G. in 1999 when she was 57 years old and had a 10-year history of type-2 diabetes mellitus. Over the years she had a difficult time controlling her blood sugar and was presently using 35 units of insulin in the morning and 20 units around dinner time.
She presented to me saying that her blood sugar was "usually" around 150 mg/dL, but that this morning her blood sugar was 361mg/dL. She added that her blood sugar was "up and down" regularly. C.G. was also taking lisinopril for hypertension and levothyroxine for her thyroid and ibuprofen for her arthritis.
Others try to help
C.G.'s ocular problems began two years earlier. She told me that for about six months before seeing an eye doctor she noticed that the vision in her right eye was getting blurry. According to C.G. (and the medical records she brought with her), the original doctors were initially worried about an optic nerve dysfunction.
After substantial testing, which included visual fields, dilated fundus examination (DFE) and magnetic resonance imaging (MRI) of the head, the previous doctors concluded that a cataract was the cause of C.G.'s 20/60 visual acuity (VA) OD. They referred her to a surgeon who performed a cataract extraction. According to her records, C.G. apparently had an uncomplicated surgery and post-op period. Her VA at the last postoperative visit was 20/25 OD, although it was noted that she was seeing a "circle inferiorly." The doctors attributed this to a mild posterior capsule opacity OD.
|
|
|
|
Red-free photo showing the
well delineated dome shape of lesion. |
|

Flash forward
Now, one-and-a-half years later, C.G.'s original optometrist refers her to me because of persistent visual blur that he can't account for with his examinations. When I asked C.G. about her surgical experience, she spun a bit of a different story, telling me that her vision got worse not long after the surgery and stayed that way. Her biggest complaint at this time was the blurred vision OD. She explained, "[It's] like there is a film in front of my eye." She also complained of seeing halos around lights, especially at night. C.G. was convinced that the cataract operation had worsened the vision in her right eye.
Stepping in
C.G.'s VA was 20/60 OD, 20/20 OS with her current spectacles and I wasn't able to improve the VA with a refraction. Her pupils were 6 mm round and reactive OU with no afferent pupillary defect. There was no pain or restriction upon eye movement. Confrontation visual fields were full OU, but C.G. did notice a "smudge" when looking at the tip of my nose with her right eye. Her posterior chamber intraocular lens was centered OD and the posterior capsule had a mild opacification.
The remainder of the slit lamp exam was normal OU. C.G.'s intraocular pressure was 10mmHg OD and 12mmHg OS. I also performed an Amsler grid test before dilation and C.G. described a central metamorphopsia OD with the lines being "doubled and jumbled" at the central 5 degrees. It was normal OS.
|
|
|
|
|
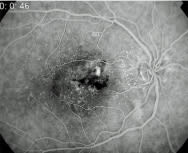
Fluorescein angiogram depicting the leakage of fluid. |

Gathering more evidence
The appearance of C.G.'s retina was not what I expected. In the fovea OD I noted an accumulation of small drusen with a definite central elevation. I didn't, however, detect any subretinal bleeding. The OS likewise exhibited central pinpoint drusen but the macula was flat. There was no diabetic hemorrhages, infarcts or exudates in either eye. I recommended an intravenous fluorescein angiography (IVFA) to help determine the true extent of the elevation and to hopefully shed some light onto its etiology.
Before I injected the dye, I looked through a red-free filter and saw that the extent of the elevation was larger than I previously thought (Fig 1). As early as 27 seconds after I injected the dye, a focal area of hyperfluorescence appeared. Peculiarly, this leakage increased only in intensity and not in size throughout the study, and the fovea "stained" sporadically (Fig 2).
Finite possibilities
C.G.'s clinical appearance was interesting, but only a few entities could create this condition. There was obviously a focal elevation at the fovea OD. The leakage on IVFA indicated either focal edema or a small subretinal neovascular membrane (SRNVM).
C.G. also had macular drusen, so the differential diagnosis was either age-related macular degeneration (ARMD), central serous choroidopathy (CSC), a pigment epithelial detachment (PED) or some combination of these. It didn't look or behave like diabetic macular edema.
|
|
|
|
Note the new area of leakage adjacent to first laser
burns. |
|
About PEDs
A PED arises because of a defect in Bruch's membrane or choriocapillaris. Serous fluid accumulates underneath the retinal pigment epithelium (RPE) layer and creates a detachment of the RPE from Bruch's membrane. The fluid causes a focal anterior displacement of the retina. PEDs seen in patients younger than 55 are generally thought of as a variant of CSC. In older patients who have PED it may be an exudative manifestation of ARMD.
Clinically PEDs can affect VA moderately (20/20 to 20/80). The location and size of the lesion and the amount of fluid all influence vision loss. Doctors will best visualize this using a 60.00D lens. The lesion will appear as a well-defined dome with rather sharp borders. IVFA is critical in making the diagnosis. A PED will show early hyperfluorescence that's sharply demarcated. It will increase in intensity but not in size.
What can you do about it?
Not all PEDs require treatment. Some do spontan-eously resolve, especially if they're smaller or in younger patients. Many don't change from their initial appearance whereas others increase in size or develop SRNVM. Base your decision on whether to treat a PED on the duration of symptoms and the likelihood of SRNVM formation. It's generally accepted that focal laser therapy be used only if the decreased VA and fluid persists beyond four to six months.
Also, treatment is more beneficial in larger PEDs and in those found in elderly patients who are more likely to develop SRNVM. If you feel treatment is warrant-ed, referral to a retinal surgeon is recommended. Treatment using a focal laser to facilitate fluid resorption should be used conservatively. Though potentially effective, focal laser therapy can also stimulate growth of a SRNVM. The surgeon must also take care so as not to place any laser burns subfoveally.
C.G. finds satisfaction
C.G. was quite bothered by her VA and after discussing the various treatment options, she chose to have laser therapy. Initially C.G.'s VA improved to 20/50, but three months after the first treatment her VA dropped to 20/200 OD secondary to a fresh SRNVM (Fig 3).
Fortunately, this lesion was juxtafoveolar and well defined so the retinal surgeon was able to treat this as well with focal laser therapy. Her eye responded quite well to the second treatment. C.G. currently has VA of 20/40 OD and 20/20 OS. She does have a small negative scotoma but says that this bothers her only "when I look for it." She hasn't had any more recurrences.
Also, though it took some time, C.G. now understands that her retinal condition wasn't caused by the prior cataract surgery!
|
CLINICAL PEARLS |
|