


CLINICAL CHALLENGES
Chronic Care
for a Chronic Case
Compassion, patience and persistence pay off when dealing with difficult patient cases.

All of us who see patients regularly care for some individuals who have conditions that, despite our best attempts, just don't seem to completely resolve. For these atypical or recalcitrant cases, we have to force ourselves to think out of the box to seek alternative therapies that may be beneficial. We also have to exhibit patience and understanding for this particular person's plight. This extended effort and thought and care won't go unnoticed by the patient, as you'll see in this particular case.
Tracing the referral path
This ongoing case began more than three years ago when an internist referred a Ms. Smith (not her real name) who was 55 years old and had been experiencing some "weird things" going on with her eyes. Two weeks before seeing me, she had seen her internist complaining of seeing flashing lights that flicker on and off and soreness in her eyes. She also told the doctor that her vision was blurred.
Her able-bodied physician measured her visual acuity (VA) as 20/20 OU in his office and didn't see any redness. He thought that he heard a bruit upon auscultation of the right carotid artery.
Because of Ms. Smith's complaints and the questionable bruit, the physician ordered a Doppler ultrasound of the carotid arteries as well as some laboratory studies. The Doppler revealed mild atherosclerotic changes but no hemodynamically significant obstructions of the carotids. He placed her on felodipine for high blood pressure, one 81 mg tablet of aspirin q.d. and referred her to me.
|
|
|
|
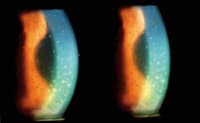
Anterior photo shows heavy accumulation of keratic precipitates
(KP) on corneal endothelium. |
|
Meeting Ms. Smith
Ms. Smith was still quite upset about the state of her eyes when I first met her. She explained to me that her eyes were still a bit sore but that the "flashes" were much better. She stated that the lights were now present only OS and that her vision seemed fine except when the lights appeared, which seemed to make her vision blurry.
I asked her to describe the eye pain more specifically and she said it was more like a dull toothache than a sharp pain. She also described the lights that she saw not as flashes but as twinkles that moved in her OS and were more noticeable at some times than others throughout the day. She seemed to be more concerned about her vision than any of the other symptoms.
Making an initial diagnosis
Ms. Smith's VA was 20/20 in each eye and her pupils were 6 mm in size, equal and reactive with no afferent pupil defect (APD). Extraocular muscle testing revealed no restriction of movement in any directions of gaze but a mild "pulling" sensation when she moved her eyes.
With a slit lamp, I saw a mild dusting of pigment on the anterior capsule of her crystalline lens OD but no overt pathology. Her OS had 1+ cell floating in the anterior chamber and mild ciliary flush. Her corneas were clear OU but I did note an early anterior subcapsular cataract OS. Her IOP measured 18 mmHg OD and 13 mmHg OS and I noted no retinal or vitreal pathology on dilated fundus examination. Specifically, there were no hemorrhages or macular edema and no disk edema. The vasculature of the retinas were normal and I saw no holes, tears or retinal detachments. I estimated her cup-to-disk ratios (C/D) at .3/.3 OD and .25/.25 OS.
I made a diagnosis of uveitis OS and explained the condition to Ms. Smith. I prescribed prednisolone acetate 1% (PredForte) OS q.i.d. and monitored her over the next two weeks. The iritis cleared as did her symptoms and I gave her a specific tapering schedule and a one-year recall.
One-and-a-half years later, Ms. Smith presented with a complaint of seeing "big, black flashes and lots of small floating dots" OU. She said that her vision was cloudy OS and that her eyes were sore. She told me that her eyes had been doing fine up until a few days ago, but that she had been having headaches for about six months. Just two months prior, a CT scan came back negative. She was now taking celecoxib as well as the felodipine and aspirin.
Searching for an answer
I measured her VA at this visit at 20/20-3 OD and 20/40 OS. Her pupils were 4 mm in size but the left was sluggish to light. I saw no APD. With the slit lamp I saw 1+ bulbar injection OU and 2+ Keratic precipitates (KP) on the cornea OU (see the photo on page 28). There were 2+ cells in the AC of both eyes and 1+ flare OU. Her IOP measured 15 mmHg OD, 13 mmHg OS. Dilated fundus exam showed a hazy view caused by the KPs, but there were no visible vitreal cells or retinal pathology.
Ms. Smith's diagnosis was now bilateral granulomatous uveitis. Because of the degree of the KP and the decreased VA, I prescribed prednisolone acetate OU q.2.h. Because this was at least her second episode of uveitis and was bilateral this time, I also ordered blood work to rule out a systemic etiology.
Ms. Smith's lab results were all negative except for a mildly elevated ESR of 38mm/hr, which was indicative of a generalized inflammatory response. Four days later, Ms. Smith's VA had improved to 20/25-2 OS and her symptoms were much better. The KPs were almost completely gone OD but were still 1+ OS. I began a slow taper of the steroid drop and I saw her each time before I tapered the drop. However, when I reduced her to b.i.d., Ms. Smith suffered a recurrence of the uveitis OS. Her VA reduced to 20/40- again and the KPs and 2+ cell and flare returned OS. Fortunately her IOP remained normal.
A long and winding road
Over the next two months, I could never get the anterior chamber reaction to completely resolve from the OS. Whenever the level of prednisolone got to b.i.d., the AC reaction flared back up and the KPs usually did too. Ms. Smith's VA was consistently 20/30 to 20/40.
I referred her to a rheumatologist because she told me her joints "ached all the time." I was hoping to get her some relief from that as well as perhaps identifying a systemic etiology for the uveitis. In addition, I suggested a more aggressive therapy for her uveitis and referred her to my ophthalmic colleague, who performed a sub-tenon's injection of triamcinolone OS and told her to continue prednisolone acetate q.i.d. OS.
|
|
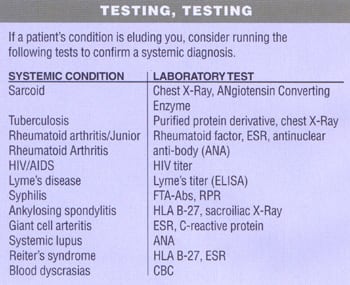
CHECKING FOR UVEITIS |
|
Order lab tests to confirm or deny uveitis in the following cases:
|
Dealing with so-so results
Ms. Smith's uveitis continues to wax and wane. I've had to place her on oral prednisone on two separate occasions to try to douse the inflammation when the uveitis recurred in the OD as well. Her VA is 20/30-2 OS because of a posterior subcapsular cataract that's developing. Fortunately, her IOP hasn't increased.
Ms. Smith gets frustrated at times -- as do I -- with our inability to completely extinguish the uveitis. She's also frustrated that none of us have been able to pinpoint a systemic cause for her problem. The rheumatologist has diagnosed her with sero-negative arthritis and has recently prescribed methotrexate in hopes of abating her rheumatologic symptoms. The methotrexate may also prove beneficial in treating the uveitis as well. I've seen Ms. Smith 11 times over the past 24 months. At her last visit, she exhibited just trace cell in the AC of both eyes and she was asymptomatic, with the exception of 20/30-2 VA OS because of the cataract.
Go ahead, get emotional
I told Ms. Smith to continue on the prednisolone acetate b.i.d. OU and scheduled a two-month recall. I may not be able to completely eradicate her inflammation, but I hope to keep it quiet more often than not. I'll continue to see her frequently and offer encouragement as well as therapeutic treatment. To Ms. Smith and to other chronic care patients, the emotional support we give is, at times, just as valuable as the medications we prescribe for them.
Contributing Editor Dr. Schmidt is director of the Bladen Eye Center in Elizabethtown, N.C. E-mail him at schmidtyvision@bellsouth.net.