


corneal reshaping
Integrating Corneal Reshaping In Your Practice
We have several options to discuss with myopes who want to wear contact lenses, but corneal reshaping has changed dramatically. Let's take a look.
BY ROBERT L. DAVIS, O.D., F.A.A.O., Oak Lawn, Ill.
With the introduction of the four- and five-zone reverse geometry GP lens designs and the awareness of refractive surgery in the consumer market, the reawakening of corneal reshaping as an alternative has changed my contact lens practice forever. I offer this procedure with confidence for patients who have prescriptions between 1.00 and 5.00. I have prescribed it in higher prescriptions with success, although I warn patients that the outcome may not reach plano, nor may it reach their expectations.
Reshaping advantages
The real advantage of corneal reshaping for the patient is not wearing contact lenses or spectacles during waking hours. Other advantages range from being able to see while engaged in water sports to no distractions during athletic activities to the cosmetic advantage to waking up in the middle of the night with adequate vision.
From the practitioner's perspective, the advantage of the corneal reshaping procedure is the industry speculation that the process has a myopia stabilization effect. Also, the wearing of a rigid contact lens in a controlled environment at night is academically the safest contact lens modality.
Reviewing the scenarios
Determine the candidacy status and the baseline for each patient at the initial visit. Exclude any patient as a candidate if he exhibits inflammation or infections of the eye including active blepharitis; any disease, injury, dystrophies or abnormality that affects the cornea or surrounding tissue; any systemic disease that may affect the eye or that could worsen by wearing contact lenses; allergic reactions of the eye, which may be caused by or exaggerated by wearing contact lenses or by the use of contact lens solutions; and eyes that are red or irritated or that suffer from severe dryness. You should discourage patients who have large pupils or a significant amount of astigmatism from this therapy option.
Initial topographical analysis will exclude corneal anomalies such as irregular corneal astigmatism, lenticular astigmatism greater than 0.75D, keratoconus and pellucid marginal degeneration. Patients who have limbus-to-limbus astigmatism as tested by topography will also have difficulty to achieve an expected result from orthokeratology. Those who have steeper corneal curvatures and higher eccentricities tend to have a better chance of success. Patients who have large pupils will suffer from halos and glare. The most important function of initial topography is to provide a baseline corneal shape from which to compare subsequent topographical changes. Follow-up topography will direct you to any necessary modifications that you'll need to make to arrive at an optimal result.
|
|
|
|
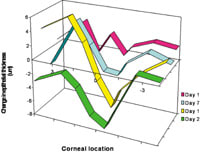
1998 Swarbrick, Corneal epithelial change with reverse geometry lenses over time. |
|
Working toward perfection
At the dispensing visit, our assistants instruct patients on proper application, removal and lens care techniques. The patient then demonstrates proper lens removal and application methods before they leave the office. Patients apply the lens immediately before bedtime. The next morning, the patient returns for a follow-up visit.
At this visit, I perform a slit lamp evaluation to check for lens movement and position. I also instill fluorescein to observe the lens-to-cornea fitting relationship, any staining or evidence of corneal abnormality. The optimal characteristic bull's-eye pattern unique to corneal reshaping exhibits a 4 mm area of central touch with 1 mm of clearance receiving the alignment curve. The fluorescein pattern, results of corneal topography and unaided visual acuity will direct lens modifications.
Our office requires that we re-evaluate patients the day after dispensing for minor adjustments and to monitor the effects of wearing the contact lens overnight. If the patient has uncorrected ammetropia after the first day, then he can wear his reverse geometry GP lens during the day or temporarily wear soft lenses until the corneal reshaping provides complete correction. Subsequent monitoring visits follow a routine of one week, two weeks, one month, two months, three months, six months and one year.
Getting down to business
Follow-up visits will monitor any corneal changes necessary for an optimal result. Our initial fee doesn't include the fitting, but it does include all visits and lens changes for an entire year unless the patient loses or breaks a lens. If I determine a lens change is necessary to achieve an optimal result during the first year, then my office will make an exchange with the patient. We insist that patients return old lenses so that they don't confuse them with the proper corneal reshaping lens.
My office expects payment in monthly installments equally divided in three-month increments. Patients can also make payments through a third-party credit company. After the first year, we employ a service agreement to cover the costs of follow-up visits. Also after the first year, we charge the patient for each replacement lens.
Trouble shooting
Each follow-up exam should demonstrate proper lens centration and a bull's eye pattern from topography. The lens position in the slit lamp may not be the same position with the eyelids closed during sleep: The upper lid forces aren't the same with the eye closed as they are with the eye open. Let your subsequent topographs direct your lens modifications to arrive at a central positioning with a minimum
4 mm treatment zone.
If the treatment zone is inferior demonstrated by a low corneal flat area by topography, the alignment curve is too steep and will occasionally exhibit air bubbles. At times, inferior positioning lenses will become immovable and will stick onto the cornea as the corneal eccentricity creates a tighter relationship than expected. As a general rule, the alignment curve controls centration. Loosen the alignment curve by .10 mm or 0.25D to improve centration.
Conversely, a superior treatment zone produced by a high riding lens is caused by a loose alignment curve. Occasionally if the lens is worn during the waking hours, the high riding lens can be triggered by tight upper eyelids. Tightening the alignment curve by .10 mm or 0.25D and/or increasing the center thickness by 0.1 mm will allow gravity to bring the lens down. Plus lenticularization will also help reduce the effect of the eyelids upon the lens.
Lateral decentered lenses are caused by a decentered corneal apex, against-the-rule astigmatism or corneal asymmetry between nasal and temporal portions. Increasing the lens diameter and adding a second alignment curve will help center the lens by creating a broader base for lens stabilization. Use alignment curve one to correspond to the temporal side and alignment two to correspond to the nasal side.
Central islands usually are indicative of vaulting over the central cornea. When bearing is present in the periphery, centrally the lens cannot bear down, causing a central island. Flattening the alignment curve or reverse curve by .10 mm or 0.25D will apply pressure evenly throughout the central cornea as the sagittal height of the lens is reduced. Increasing the amount of central touch will alleviate poor vision related to central islands. At times a tight reverse curve can cause central vaulting. Loosening the reverse curve by .20 mm or 0.75D will cause the lens to bear down centrally.
Corneal staining is a sign of either mechanical irritation or physiological problems requiring immediate remediation. A tight lens will trap material under the lens with no tear exchange. Increase fluid exchange by loosening the peripheral curve and/or the alignment curve to remediate the tight lens syndrome. Air bubbles from vaulting over the central cornea or the reverse zone will cause dimple veiling. A base curve that is too flat increases the mechanical pressure onto the cornea, creating a rubbing action on the corneal apex and developing an abrasion.
Patients on dehydration medications can also create a tear insufficiency problem. Punctal occlusion has resolved many problems related to poor tear volume. Midperipheral arcuate staining refers to a tight peripheral curve design. Loosen the peripheral curve or design an aspheric peripheral zone system to alleviate the problem. A lens polymer creating corneal hypoxia can result in physiological distress and corneal staining. Solution toxicity can always stain and masquerade as a hypoxic or mechanical problem. A solution toxicity problem will generally be immediate.
Corneal indentation. When lens pressure is applied onto the cornea an indentation or distortion will show up as a lens imprint. This unwanted result is caused by a reverse curve that's too tight or a decentered lens creating an undesired contact lens-corneal relationship. Some corneas are just soft and a lens imprint is normal. Loosen the alignment curve and/or reverse curve by .15 mm or 0.50D to ease the problem.
Under responders and over responders are patients who react in an unpredicted manner. These are the only scenarios that warrant a base curve change. Flatten or steepen the central base curve by half diopter increments to arrive at the appropriate prescription providing that the fluorescein pattern is normal. If the uncorrected visual acuity doesn't hold for an acceptable amount of time, then the central bearing pressure isn't being applied centrally. The usual cause is a slightly decentered lens position.
The sagittal height of the reverse curve is too low, resulting in no space for the central tissue to be displaced. Increasing the sagittal height or steepening the reverse curve allows more space for the central tissue to relocate. Fluorescein pattern will exhibit a wider alignment zone. Some patients' corneas are rigid and will not be affected in a predictable behavior.
Ghosting at night usually occurs when the pupil dilates and the treatment zone is smaller than the papillary size. Increasing the treatment zone to 6.2 mm will usually solve this problem. Patients who have uncorrected astigmatism will also complain of ghosting. Increasing the central baring by reducing the sagittal height through the reverse curve and alignment curve usually will improve this distortion.
Stuck lenses. In the morning, lenses sometimes get stuck centrally on the cornea with no lens movement, resulting in central staining and lens imprint. This will result in an inadequate tear supply solved by punctual occlusion. Lubrication drops will prime the lens, improving the lens to float on the cornea and maintaining an ample tear exchange. Loosening the reverse curve will also cause better tear movement so the lens doesn't get locked down onto the cornea. At times a change in one parameter will cause a change in the corneal/lens relationship. Flattening the reverse curve might mandate a change in the alignment curve to maintain lens centration.
Embrace corneal reshaping
The objective of corneal reshaping is to provide safe, overnight contact lens wear that creates a predicted refractive change and provides clear vision throughout the day without lens correction. Overnight lens wear provides a convenient method of corneal changes, improved lens tolerance without lid interaction and reduces symptoms of daytime dryness.
The benefits for recreational activities without wearing a contact lens dramatically change the way GP lenses are perceived --there's no longer the fear of grit getting under the contact lens, lens displacement or drying effects of wind. Recent advances in GP lens polymers allows initial all night lens wear without establishing an adapted lens wearing schedule.
The advent of modern corneal shaping lens designs has moved this procedure into mainstream contact lens treatment plans. The advantages of this modality over other contact lens devices (not wearing lenses or spectacles during waking hours and its myopia stabilization effect) mandates that contact lens practitioners learn this technique as a viable procedure option therapy.
Dr. Davis is in private practice and conducts clinical research. He's a diplomate in the Cornea and Contact Lens Section of the American Academy of Optometry.5