


dry eye
Emerging Trends in Dry Eye Management
Clinical pearls for the diagnosis, treatment and management of this ocular surface disease.
BY KENNETH LEBOW, O.D., F.A.A.O., Virginia Beach, Virg.
Diagnosing dry eye disease is a complex and multifactorial process. In an attempt to make this process a little easier, this article will review some of the emerging trends in the diagnosis, treatment and management of the dry eye patient.
|
|
|
|
|
|

|
|

|
|
|
PHOTOS BY PAT SIMIONE |


How it all begins
The National Eye Institute (NEI) Workshop classifies dry eye into the following etiologies:
- tear deficient (Sjögrens and non-Sjögrens disease)
- evaporative (oil-deficient lid-related, contact lens- or surface change-induced).
However, additional factors (aging, external environmental changes, systemic medications, ocular surgery, chronic blepharitis or meibomianitis) can further complicate the diagnosis. Inflammation and tear film hyperosmolarity are also major components that experts associate with this disorder. In some contact lens situations, otherwise asymptomatic contact lens wearers may report dryness only when wearing their lenses. Other obstacles get in our way, as I'll explain.
Hurdles to anticipate
A significant problem with dry eye is that patient signs and symptoms often don't correlate. It's not unusual for one patient to report significant symptoms such as burning, scratchiness and stinging, but to not demonstrate clinical signs of conjunctival hyperemia, reduced tear break-up time (TBUT), corneal or conjunctival staining. At the other extreme, some patients may claim that they're virtually symptom-free, yet they manifest significant corneal and conjunctival involvement. Patients may also show both signs and symptoms but these may not be consistent from patient to patient.
Moreover, researchers have associated pro-inflammatory mediators such as cytokines and leukotrines with an inflammatory component of dry eye. Because of this significant dichotomy between signs and symptoms, practitioners frequently diagnose dry eye solely on the basis of patient-reported symptoms in response to dry eye questionnaires. And, when a patient reports dry eye symptoms in the absence of clinically demonstrable signs, more often than not, a practitioner will consider him to have a dry eye problem.
Bucking tradition
One of the more significant emerging trends in our understanding of dry eye disease calls into question the traditional description of the tear film as distinct monolayers: mucin, aqueous and lipid.
The established view of dry eye disease links mucin deficiency with non-wetting and surface damage, aqueous deficiency with keratoconjunctivitis sicca or "true" dry eye and meibum deficiency with evaporative dry eye. A more contemporary model of the human tear film describes the tears as being in aqueous phase throughout their entire thickness with varying concentrations of different types of mucins located in different areas.
For example, mucins 1, 4 and 16 (MUC1, -4 and -16) are transmembrane mucins associated with the corneal and conjunctival epithelial layer and help develop the glycocalyx. MUC5AC is a gel-forming mucin released from goblet cells that's typically found in the substance of the aqueous of the tears while MUC7 from the lacrimal gland is a more soluble type of mucin. Clearly, these different mucins play diverse roles in the stabilization of the tear film, reduction of evaporative effects and the protection of the ocular surface. Check out "Know Your Mucins" below for a simple overview.
Another concept gaining acceptance in the industry and among practitioners is that the tears are like a living ocean comprised of the ocular surface, glycocalyx and three tear zones. The eyelids are the equivalent of the land surrounding the ocean of tears and can create motion that affects the stability of the tear film. Deficiency in any component of the ocular surface environment can lead to a compromised tear film, which in turn causes cellular damage. In addition to mucins and the tear film, the role of glycocalyx in ocular surface disease (OSD) is an important factor in dry eye patients.
|
|
|
|
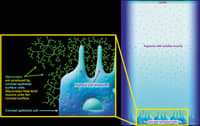
Fig. 1: A theoretical example of glycocalyx. |
|
Glycocalyx and OSD
Scientists describe glycocalyx as a cotton candy-like structure that the epithelial surface cells produce to trap mucins to the microvilli on the ocular surface. They also associate disruption of the glycocalyx with tear film instability. Figure 1 provides a theoretical example of glycocalyx.
A damaged glycocalyx exposes the epithelial cell, resulting in a loss of microvilli. Loss of trans-membrane mucins such as MUC1, -4 and -16 ultimately expose the underlying, inherently hydrophobic corneal surface, which causes destabilization of the tear film with the development of dry spots as evaluated with vital dyes. Once exposed, the corneal surface loses the protection of an intact tear film. Then it's up to us to determine the severity of a patient's condition.
Making the call
The McMonnies Index, Candees and the Ocular Surface Disease Index (OSDI) are dry eye questionnaires, but practitioners don't just use them to identify dry eye patients; they've incorporated them to evaluate the success of therapeutic intervention providing a readily quantifiable assessment of patient response to therapy.
|
Know Your Mucins |
||
| MUCIN | FUNCTION | LOCATION |
| MUC1, -4, -16 | Membrane-bound mucins | Corneal epithelial surface |
| MUC5AC | Gel-forming mucins | Dissolved within the aqueous |
| MUC7 | Soluble mucins | Associated with outer lipid component of aqueous |
Protecting the ocular surface
The goal of all dry eye therapies is to maintain a protected ocular surface. Blinking is one mechanism that helps spread the tear film over the ocular surface and re-establish its integrity. However, an open eye exposes itself to various atmospheric factors that exert an additional evaporative force on the tear film, reducing its volume and increasing the exposure of the ocular surface to damage and desiccation.
|
|
|
|
|
Fig. 2: An example of tear break up. |
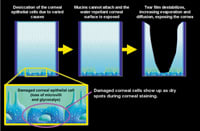
A protected ocular surface will exist as long as the tear film remains stable. Once tear film break up occurs (before the next blink re-distributes the tear film) the ocular surface is at risk of corneal damage. Repeated exposure to reduced TBUT between blinks can result in corneal staining and patient reports of ocular discomfort.
The Ocular Protection Index (OPI) represents another emerging trend in managing dry eye disease and helps to quantify this phenomenon. An OPI of greater than 1.0 represents a tear-protected ocular surface. Conversely, an OPI of less than 1.0 depicts an unprotected ocular surface with exacerbated signs and symptoms.
For a review of treatment strategies geared toward dry eye disease, see "Dry Eye Treatment Tactics" beginning on page 35.
Put some thought into it
Although dry eye disease is a chronic condition that can defy treatment, it requires a logical therapeutic approach. Our ultimate goals in treating dry eye disease should include regeneration of epithelial cells, reductions in signs and symptoms of dry eye and the establishment of a healthy ocular surface.
References available on request.
|
Dry Eye Treatment Tactics |
| With new research, therapies and drug combinations, today's optometrists have a greater capacity to diagnose and treat the millions of dry eye sufferers, including those who have severe dry eye. Below, Optometric Management presents two approaches to the management of dry eye. Progressive treatment For mild dry eye, over-the-counter (OTC) drops are still the best choice, says Kenneth Lebow, O.D., F.A.A.O. Initial therapy should revolve around stabilization of the tear film using lubricant eye drops that have demonstrated clinical efficacy. Dr. Lebow cites three lubricating drops: 1. Systane Lubricant Drops (Alcon Laboratories) forms a soft gel matrix in the eye that has bioadhesive properties binding to the glycocalyx, protecting desiccated epithelial cells as well as attaching to the lipid layer to help reduce evaporation. 2. Refresh Endura Lubricating Eye Drops (Allergan) contain emulsion structures that are released by electrolytes naturally found in the tear film so that the oil component of the lubricating drops subsequently floats to the lipid layer, the water content enhances aqueous volume and the ocular lubricant combines with the mucin layer. 3. "Soothe Emollient Eye Drops (Alimera Sciences), which contains an advanced lipid restorative, creates a metastable emulsion in an aqueous base," he adds. "The next step in the process," he says, "should involve pulse-treatment (for two to four weeks) with a low-dose soft steroid such as Bausch & Lomb's Alrex (loteprednol etabonate ophthalmic suspension 0.2%)" He further adds that successful remediation of symptoms with a steroid is a good indication that Restasis (cyclosporine ophthalmic emulsion, 0.05%, Allergan) with Systane as concomitant therapy is the next longer-term approach to treatment. "Ultimately," Dr. Lebow suggests, "punctal occlusion may also be required to minimize patient symptoms and to repair corneal damage." Treating one level at a time Paul Karpecki, O.D., F.A.A.O., follows the results of a Delphi panel approach led by the Wilmer Eye Institute. Here, he shares their recommendations: ► The first level of severity consists of mild to moderate symptoms and signs and suggested treatment includes preserved tears, allergy drops, lifestyle changes and environmental management. ► Patients who have level two severity have moderate symptoms, tear film and visual signs and conjunctival and mild corneal punctuate staining. The panel recommends unpreserved tears, gels or ointments, corticosteroids or Restasis. ► The third level demonstrates severe symptoms, marked corneal punctuate staining, central corneal staining and filamentary keratitis. This level requires more aggressive treatment with Restasis, punctal plugs, tetracycline or topical steroids. ► The fourth level of dry eye consists of severe symptoms and corneal staining and erosions and conjunctival scarring. While patients may respond to Restasis at this level, they often require surgery, punctal cautery, acetylcysteine or contact lenses. Seventeen international dry eye experts participated in the panel to develop modern treatment recommendations for different types and severity levels of dry eye disease. Says Dr. Karpecki, "Treatment algorithms are often complicated, especially when multiple treatments and strategies are available for one single disease and for different stages of that disease. Until now, there was no clear approach to treating dry eye or to assigning therapeutic recommendations as 'first,' 'second' or 'third' line, which is why these recommendations are monumental." According to the panel experts, patient symptoms include use of tears, ocular discomfort or fatigue and visual disturbance. The presence of clinical signs in the lids, tear film, conjunctiva, cornea and vision were deemed most relevant in categorizing the severity of a patient. Therapies on the horizon Dr. Lebow reviews some other categories of therapeutic agents designed to treat dry eye disease that are on the horizon: "Secretagogues stimulate mucin production and in spite of initial unsuccessful attempts to gain FDA approval, a collaborative effort between Inspire Pharmaceuticals and Allergan will hopefully bring diquafosol (INS365, a P2Y2 agonist) to market," he says. Researchers expect INS365 to work on receptors found on epithelial cells stimulating mucin, lacrimal secretion and possibly lipid production. Dr. Lebow adds that another secretagogue that's selective for MUC1 is Alcon's 15-(S)-HETE (hydroxyeicosatetraenoic acid), which is also under investigation. "Additional mucomimetics and demulcents under research include Vista Scientific's mucomimetic Milcin, which incorporates into the mucin layer and mimics secreted mucin; and Pfizer's hyaluronic acid-based demulcent and the company's derived mucomimetic Quinolone," reports Dr. Lebow. He says that scientists are also considering new anti-inflammatory applications for low-dose steroids and cytokine inhibitors as additional treatments for dry eye disease. |
