


|
|
|
Coordinated by Bobby Christensen, O.D., F.A.A.O. |

therapeutic insights
Looking Out for DLK
If you co-manage LASIK patients, be aware of this uncommon but significant complication.
By Neha Patel, O.D.
With the increasing popularity of LASIK refractive surgery, it's important for eyecare practitioners to be aware of both the common as well as the uncommon complications associated with this procedure. In 1998, Smith and Maloney first reported a significant complication of post-LASIK: a noninfectious inflammatory reaction occurring in the lamellar interface of the flap occurring primarily in the first week after the LASIK procedure. They termed the condition diffuse lamellar keratitis (DLK). Those of us who are active in the postoperative care of refractive surgery patients must remember that prompt recognition, diagnosis and management is critical for a successful outcome.
Meet DLK
Experts clinically describe DLK, also known as "Sands of the Sahara," as a diffuse granular or powdery inflammatory haze at the level of the interface. Symptoms may include reduced vision, photophobia, redness and pain, depending on the severity of the condition. The conjunctiva is typically not inflamed and there is little to no anterior chamber activity.
The reported incidence of DLK differs widely; some have suggested that mild cases may affect as many as one in 50 patients, while severe presentations of DLK are much less common with one in 5,000.
|
|
|
|
|
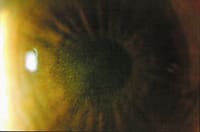
Figure 1: Stage 2 DLK |
|
|
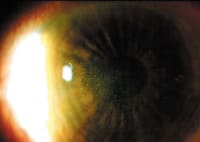
| Figure 2: Close up view of white granular cells in the center of the flap and flap periphery in Stage 2 DLK. | |

|
|
| Figure 3: The optic section of the cornea showing white granular cells in the interface of the flap. |
The stages of DLK
The typical time of onset of DLK is within one to six days following surgery, with many cases being observed on day 1 postoperatively. Once you identify DLK, it's essential to determine its severity and location, as this will direct the treatment modality. Depending on when you identify DLK, it can present in any of the following stages.
Stage 1. White granular cells seen in the periphery of the lamellar flap with no involvement of the visual axis.
Stage 2. White granular cells seen in the center of the flap involving the visual axis and the flap periphery.
Stage 3. Clumping of cells at the visual axis causing reduced vision and haze.
Stage 4. Central stromal necrosis and corneal melt with induced hyperopia and corneal astigmatism.
The histopathology of DLK has shown to be a dense infiltration of round, white blood cells at the level of the LASIK interface. On post-op day 1, white blood cells encroach the flap peripherally. Usually on day 2 the cells will migrate toward the central part of the flap, giving a shifting sands appearance. With further progression, the cellular reaction will intensify, causing central clumping of cells. If untreated, this will lead to permanent scarring and stromal melting. Thus, experts consider DLK a threshold disease.
Most often, we see DLK on day 1 postoperatively; however, we'd see the peak cellular reaction on day 5 or 6. Nonetheless, some clinicians report observing DLK six months postoperatively -- this is also known as late-onset DLK. It's mostly associated with an epithelial defect or with eye trauma.
Keeping an eye on it
The appearance of DLK closely mimics multifocal infectious infiltrates, thus it's important to rule out this etiology. Infectious keratitis is typically focal rather than diffuse. In addition, infectious keratitis is associated with pain, conjunctival injection and discharge. The corneal involvement in infectious cases isn't confined to the interface but may penetrate into the corneal stroma in contrast to DLK, which tends to only involve the flap interface. If you can't make a definitive diagnosis, then lift the flap and take cultures. Treat the condition as infectious until proven otherwise.
Where does it come from?
Science doesn't yet know the etiology of DLK. Doctors have suggested a variety of possible etiologies and many have concluded that DLK may in fact be multifactorial. Possible etiologies include microkeratome oil, metallic debris from the microkeratome blade, bacterial endotoxins, meibomian gland secretions and epithelial defects.
Shah and coauthors showed that epithelial defects increase the risk of DLK by up to 24 times in the early postoperative period. Stage 1 DLK may be caused by an increased inflammatory response that comes from normal surgical trauma of the LASIK procedure. This leads to the idea that Stage 1 DLK patients have a more intense wound-healing process, causing visible inflammation, than what would be seen in most patients with a subclinical inflammatory reaction.
Stage 2 DLK is more aggressive than Stage 1 and is likely caused by the agents that I've previously stated. The duration until resolution and the risk of losing vision can be significantly greater with Stage 2 DLK.
Getting a plan of attack
The principal treatment for Stages 1 and 2 DLK is aggressive use of topical steroids, usually prednisolone acetate 1% every hour with suggestion of using dexamethasone 1% steroid ointment at night, although no randomized study has concluded this to be of benefit. Prompt follow up in 24 to 48 hours is necessary to identify the few cases that will progress to Stage 3. Stages 1 and 2 follow a self-limited course and the majority of cases resolve in seven to 10 days.
It's essential to be cautious of acute IOP rise secondary to potent high-dose topical steroid therapy. And take careful consideration of the pressure in thinner post-LASIK corneas. Applanation and Tono-Pen will underestimate the IOPs, so it's best to compare pretreatment IOP with post-treatment IOP to determine the steroid responders. Treat steroid responders with less potent topical steroid formulations.
Treatment of Stages 3 and 4 DLK involves lifting the flap and debulking the inflammatory debris with irrigation of the bed and undersurface of the cap. Research shows that it's most effective to lift the flap 48 to 72 hours after the initial procedure. However, some reports suggest that lifting the flap with Stage 4 DLK is of little benefit and may add to stromal volume loss. For patients who have a less-than-optimum response to topical steroid therapy and who have more severe presentations, consider using oral prednisolone as an adjunct therapy.
Just in case
Most patients respond well to treatment, but for those who regress, there's the possibility that they may end up with an irregular flap and induced irregular astigmatism. In these cases, a GP lens may prove beneficial for increasing visual function. Surgical options can include phototherapeutic keratectomy (PTK). Rarely, if there is corneal scarring and marked corneal irregularity, a penetrating keratoplasty may be indicated.
Stay on top of it
DLK is a significant complication of LASIK, with a multifactorial etiology. Optometrists who are involved with post-op refractive surgery patient care should be aware and able to correctly identify this condition. Prompt treatment and management will ensure the most favorable patient visual success.
References available on request.
Dr. Patel is a resident at the Bascom Palmer Eye Institute in Miami. Contact her at npatel@med.miami.edu.
Dr. Christensen has a partnership practice in Midwest City, Okla. He's a diplomate in the Cornea and Contact Lens Section of the American Academy of Optometry. He's also a member of National Academies of Practice.