


glaucoma
Treating
Glaucoma: The Role of
Selective Laser Trabeculoplasty
Understand
the basics of this therapy to choose the best option for your patients.

Which is appropriate as a first line treatment for your glaucoma patients: medication or surgery? We know that medications are only helpful when patients take them, but they often don't. Patients don't adhere to treatment for a number of reasons including inconvenience, lack of perceived benefit, cost, forgetfulness and adverse side effects. And even when patients do use their medications, they often do so inappropriately. This results in fluctuations in intraocular pressure (IOP) and can ultimately result in glaucomatous progression.
Surgical procedures have been suggested as a way to reduce the "patient compliance factor" in glaucoma treatment. The seven-year results of the Glaucoma Laser Trial (GLT) show patients who were initially treated with argon laser trabeculoplasty (ALT) had lower IOPs and slightly better visual fields and optic nerve preservation than patients who were treated with medications first. In clinical practice, however, few patients elect initial laser treatment when given the option.
But recent developments in laser technologies are giving patients something new to think about and provide another option for you to discuss with them. Selective laser trabeculoplasty (SLT) has been shown to be as effective as ALT for patients with open-angle glaucoma and can even be offered to those with poor IOP control and previous ALT.
|
|
| Comparison of spot size for ALT (right) and SLT (left). |

Surgical primer
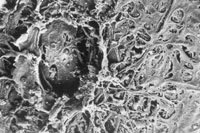
ALT uses a blue-green laser to create thermal burns in the trabecular meshwork (TM). This laser uses a relatively small spot size (about 50nm) of varying intensity to photocoagulate the TM (see image on page 63). It's a non-selective laser that creates crater-like depressions and transfers thermal energy to nearby TM structures. The collateral damage caused to all surrounding tissues results in the rupture of trabecular beams and collagen supporting structures, scattered debris and fibrosis (see image at left). ALT is thought to reduce IOP by mechanical and/or biologic mechanisms. The mechanical theory is based on the idea that the laser burns cause the TM to contract in the area of the burn and the structures adjacent to the TM to widen, allowing for increased outflow. The biologic theory involves the recruitment of macrophages and the increased phagocytic activity of trabecular cells.
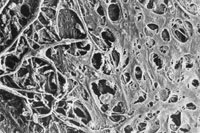
SLT uses a Q-switched, frequency-doubled, Nd:YAG laser to selectively target the melanin-containing cells of the trabecular meshwork or selective photo-thermolysis. The 532nm laser energy is delivered over a short pulse duration of three nanoseconds, which produces little collateral damage to adjacent TM. The spot size measures 400nm. A very small amount of energy (0.6 to 0.9 mJ) is applied over a relatively large area in SLT, but because the power settings are so low, there isn't enough energy to convert the electromagnetic power in the TM melanosomes into thermal energy. Only pigmented TM cells are disrupted; surrounding tissues are preserved (see image on page 66). SLT is thought to release cytokines and other chemicals that stimulate the recruitment of macrophages, which help to phagocytize TM debris to improve outflow.
Comparing SLT with ALT
|
|
| Scanning electron microscopy of ALT treatment. |
Studies have shown SLT to be as effective at IOP reduction as ALT in patients with uncontrolled open-angle glaucoma or ocular hypertension. This technique has been used in eyes that have been previously treated with ALT. One study reviewing the current literature found SLT achieved an average IOP reduction of between 3.9mm Hg and 8.0mm Hg. Patients who underwent SLT after ALT achieved about the same level of reduction as those who underwent SLT as a first line procedure. Patients also seem to tolerate SLT better than ALT, with a lower degree of post-operative inflammation and less discomfort. SLT patients also experience fewer postoperative IOP spikes compared with ALT — a finding attributed to SLT delivering only 1% of ALT's energy.
There has been considerable excitement surrounding SLT in the ophthalmic community. Although typically used as adjunctive therapy, a preliminary report suggests that SLT may be a safe and effective primary intervention for glaucoma and ocular hypertension. But further data is needed to determine whether SLT is a better first line option than medical therapy. A 12-month prospective, randomized, controlled, multi-center study is currently underway (SLT/MED study).
The five-year data from studies that are currently available show a progressive loss of effect in SLT, meaning increasing treatment failure over time — similar to that seen in patients with ALT. It is estimated that 50% of patients treated with ALT will maintain IOP control at five years post-treatment, with a loss of 6-10% per year thereafter. And patients with lower baseline IOP were found to be at greater risk for treatment failure compared with those who had higher pre-treatment pressures.
Whether SLT will provide better long-term IOP control than ALT is not yet known. Advise patients who elect SLT that there is a significant likelihood that additional treatment may be necessary over time.
There is some controversy regarding the optimum parameters for SLT. Some reports suggest that a 90Þ treatment is as effective as a 180Þ treatment, whereas others suggest that both 180Þ and 360Þ treatments are better than 90Þ treatments. There is no defin-itive data to show that one protocol is better than another. Factors such as efficacy, risk of post-operative complications, convenience and likely return for follow-up may all play a role in the surgeon's decision.
Future research should evaluate the efficacy of repeat SLT treatments, since there is limited information about this application in the current literature. It has been proposed that SLT is repeatable, given there is no thermal damage to the TM. However, further study is necessary to confirm this.
|
|
| Scanning electron microscopy of SLT treatment. |
Other pearls
Patients who have uncontrolled primary open-angle glaucoma may benefit from SLT. This procedure is contraindicated in patients with a history of congenital, inflammatory, neovascular or traumatic glaucoma, primary or secondary angle closure, or other conditions that would preclude adequate view of the TM. Compliance is key, so elderly patients who may have difficulty with drop instillation or medication cost may not be the best candidates for SLT. Younger patients, however, find this new technology appealing and may be interested in SLT as a way to simplify their regimen.
Post-operative complications occur infrequently after SLT and include conditions such as a post-operative pressure spikes or iritis. We prescribe prednisolone acetate 1% (Pred Forte, Allergan) drops q.i.d. for four days after the procedure to prevent inflammation. Others recommend a topical NSAID q.i.d. for four to seven days or may use no post-operative medications at all. Our surgeons found that patients who do not receive post-operative anti-inflammatory medications develop iritis more often.
SLT is billed as trabeculoplasty by laser surgery, one or more sessions (CPT 65855). It's considered a "minor" procedure with a global period of ten days, which is generally not comanaged. The patient will typically follow-up with the surgeon within the first four to seven days post-op. He or she should then follow-up in the O.D.'s office approximately four to six weeks later. Instruct patients to maintain all current topical medications until at least six weeks after the procedure. Reverse trials may be attempted thereafter, if IOP levels demonstrate good response. However, for most patients, SLT is an additive therapy and therefore medications will remain unchanged.
| The Basics — Comparison of SLT and ALT | ||
|
Parameter |
ALT | SLT |
| Laser | Argon blue-green | Q-switched, frequency-doubled Nd:YAG |
| Wavelength | 514 nm | 532 nm |
| Spot size | 50 mm | 400 nm |
| Duration | 0.1 s | 3 ns |
| Parameters | 400-1000 mW | 0.6-0.9 mJ |
| Laser activity | Photocoagulation | Selective photothermolysis (SP) |
| Selectiveness | Non-selective | Pigmented TM only |
| Mechanism of IOP reduction | Mechanical, biologic | Biologic |
SLT can give you another tool to manage glaucoma — particularly for those patients with uncontrolled IOP in whom medical alternatives have failed, those who cannot tolerate medications or decline incisional surgery. SLT can effectively lower IOP in patients with or without a history of failed ALT, using considerably less energy and causing less thermal damage to the TM. However, we still need more infor- mation about the role of SLT as a primary procedure, its long-term effectiveness and the efficacy of repeated procedures.
References available upon request.
Optometric Management is proud to present this first in a series of articles on glaucoma that have been planned in partnership with the Optometric Glaucoma Society (OGS). In 2006, the Society will provide OM with expert authors who will discuss therapies, epidemiology, case studies and other current issues in glaucoma management. For additional information on the Society, contact the OGS through the Web site optometricglaucomasociety.org. The views expressed in this article are the author's and do not necessarily represent the views of the OGS.
Dr. Yang-Williams is on staff at Northwest Eye Surgeons in Seattle and serves as adjunct Clinical Faculty for Pacific University College of Optometry. She is also a member of the Optometric Glaucoma Society Executive Board.