


Optimizing the Management Of Dry Eye Inflammation
An expert discusses the potent, synergistic effect that makes combination therapy the preferred choice for battling inflammation.
By Paul M. Karpecki, O.D., F.A.A.O.

Dry eye syndrome, or keratoconjunctivitis sicca, represents about 25% of all patient visits to eyecare professionals.1 Up to 40 million Americans have symptoms or risk factors for the disease.2 Half of patients over age 65 and one-third of women between ages 40 and 59 have symptoms.3
Yet, despite the prevalence of dry eye, it's still considered one of the most underdiagnosed4 eye diseases because of its various underlying causes, complex symptoms and our previously limited knowledge of its pathogenesis.
For years, we advised patients to use artificial tears as their primary treatment, or we suggested they switch to a higher viscosity lubricant. Often, punctal plugs were a last resort. Today, these same patients continue to treat themselves with over-the counter lubricant eye drops that provide unsatisfactory relief. And they're unaware of the alternatives. Annual sales of artificial tears in the United States are nearly $150 million.5
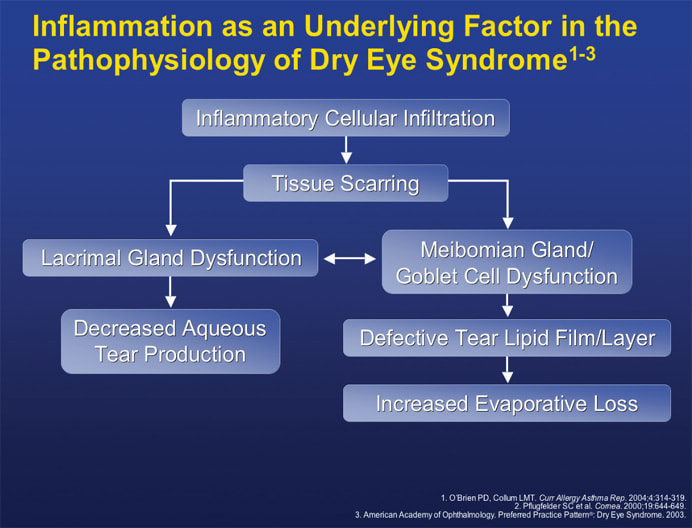
An inflammatory cellular infiltration can lead to lacrimal gland dysfunction, decreased aqueous tear production, meibomian gland/goblet cell dysfunction and evaporative loss.
Our limited understanding of dry eye etiology over the past several years has hindered how we treat our patients. We've been less inclined to diagnose and treat dry eye aggressively because of its ubiquitous nature and the fact it's a chronic problem. However, our understanding of dry eye has evolved. We now know it has an inflammatory component. And if the inflammation is left untreated, it can significantly damage the ocular surface.
This article will discuss the underlying inflammatory nature of dry eye, the importance of early diagnosis and the efficacy of combination therapy — a fresh approach to managing the disease.
An inflammatory disease
Over the years, we've come to realize that dry eye is an ocular surface inflammatory disease. We always understood that people with dry eye had either low tear volume due to rapid evaporation or inadequate tear production. We've now learned how low tear volume compromises the ocular surface and weakens its protection against external elements. Low tear volume also affects the quality of tears, changing their osmolarity and triggering red an inflammatory response.

Significant inferior superficial punctate keratitis in a patient complaining of burning eyes.
Many studies have shown the important role of inflammation in the pathogenesis of dry eye,5–9 and human and animal models have illustrated the role T-cells and other inflammatory mediators play in the disease.8–11
| We now know that [dry eye disease] has an inflammatory component. And if the inflammation is left untreated, it can significantly damage the ocular surface. |
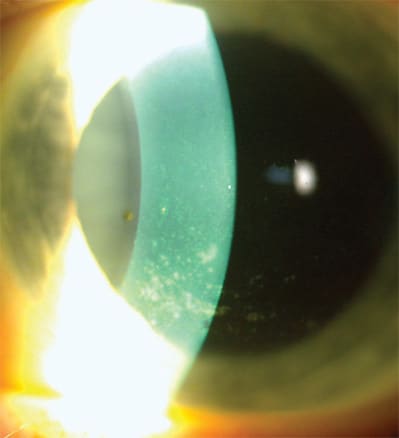
A 51-year-old Caucasian female with marked corneal staining and filamentary keratitis.
Without sufficient tear volume, the complex biochemical structure of tears changes, and these changes lead to a higher concentration of inflammatory cells and other mediators in the tears, causing inflammation.6 Typically, this inflammatory process is cyclical and, therefore, chronic. It won't resolve on its own. Abnormal tear film composition, production and rapid evaporation perpetuate the inflammatory cycle.4 And inflammatory cellular infiltration can lead to lacrimal gland dysfunction and decreased aqueous tear production, meibomian gland/goblet cell dysfunction, a defective lipid layer in the tear film and greater evaporative loss.1,7
Once researchers demonstrated the inflammatory and cyclical nature of dry eye syndrome, all the pieces of the puzzle seemed to come together. Now, we realize that the signs and symptoms of dry eye, such as redness, burning, stinging and light sensitivity, are consistent with inflammation. As final proof, these signs and symptoms respond well to anti-inflammatory drugs.
| Several tests are available to evaluate dry eye symptoms, but none will provide a definitive diagnosis, so we rely primarily on patients' self-reported symptoms. |
Thorough testing
Several tests are available to evaluate dry eye symptoms, but none will provide a definitive diagnosis, so we rely primarily on patients' self-reported symptoms. Inflammation often is present long before clinical signs appear, so there may not be much correlation between the two.1,12 Nevertheless, the risk of ocular complications from untreated inflammation makes early diagnosis imperative.
The tests include:
■ History, including questions about the health of the ocular surface
■ Clinical exam
■ Schirmer test
■ Fluorescein tear breakup time
■ Ocular surface staining with rose bengal, lissamine green or fluorescein dye.
Based on these test results, you can follow the recommendations of the Dry Eye International Task Force to stage patients with dry eye, ranging from level one to level four. These criteria will help you choose the best treatment.
Treatment options
Treatment options for dry eye include over-the-counter artificial tears, loteprednol etabonate ophthalmic suspension 0.5% (Lotemax), cyclosporine ophthalmic emulsion 0.05% (Restasis), oral doxycycline and omega-3 supplements, moisture chambers and goggles, and in severe cases, punctal plugs or tarsorrhaphy.
By the time my dry eye patients come to my office, most of them already have used an over-the-counter lubricant for quick relief, so I focus on treating the disease. If they haven't tried anything yet, I prescribe an artificial tear and suggest lifestyle and environmental changes, such as avoiding caffeine and alcohol, and steering clear of dry air from ceiling fans and heating vents.
If a patient's dry eye doesn't respond to these measures, my goal is to reduce the inflammation. I'll prescribe an anti-inflammatory/immunomodulatory combination of loteprednol 0.5% and cyclosporine drops. Each drug has its advantages and limitations, but their effects are complementary when used together. The loteprednol reduces burning and stinging, provides immediate symptom relief and is safer than other steroids. The cyclosporine provides long-term safety and efficacy. I prescribe loteprednol 0.5% first four times a day for 2 weeks followed by twice-a-day dosing for 6 weeks, then p.r.n. for what remains in the bottle. I prescribe cyclosporine 0.05% two times a day for 6 months. And after 6 months of effective antiinflammatory treatment, I may recommend omega-3 fatty acid supplements along with cyclosporine drops long-term for patients with chronic dry eye.
In rare cases when significant lid disease is present, I prescribe low-dose oral doxycycline (50 mg or 20 mg twice a day) to patients who don't respond to safer topical anti-inflammatory agents, or if they have acne rosacea. I discuss the advantages of making dietary modifications with the patient, such as eating more fish high in omega-3 fatty acids or taking supplements.
Pros and cons: cyclosporine and corticosteroids
Cyclosporine is an immunomodulator that suppresses T-cells, inhibits their activation and downregulates T-cell mediated cytokines.1,12–14 In a large, randomized, 6-month, multicenter study comparing cyclosporine drops to placebo for treatment of moderate to severe dry eye, patients treated with the immunomodulator twice a day were more likely to have better Schirmer results after 6 months (15% compared to 5%).14
| In rare cases when significant lid disease is present, I prescribe low-dose oral doxycycline (50 mg or 20 mg twice a day) to patients who don't respond to safer topical anti-inflammatory agents, or if they have acne rosacea. |
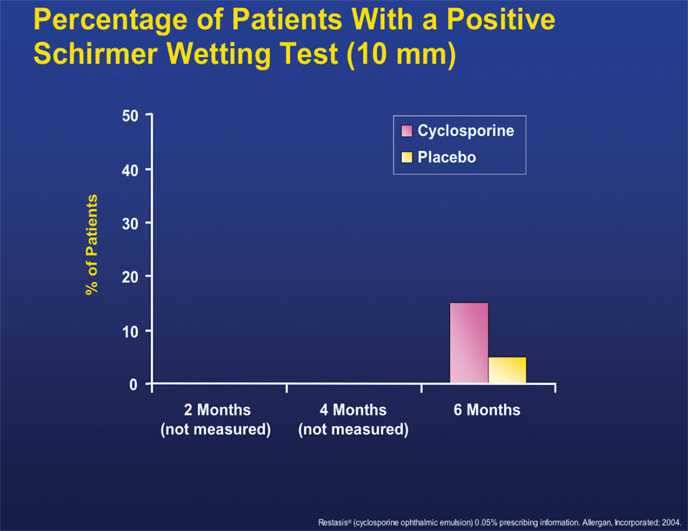
In a large randomized, multicenter study, patients treated with cyclosporine 0.05% twice a day for moderate to severe dry eye were more likely to have better Schirmer results after 6 months.
Seventeen percent of patients treated with cyclosporine complained of burning — a limitation of the drug and the most common adverse event in this study.
Today's broad-spectrum, topical corticosteroids have a mechanism of action that interrupts the inflammatory response at key, early stages of the disease. They limit production of inflammatory precursor proteins at a nuclear level and control the increase of mast cells and lymphocytes at the cellular level.15 Biochemical actions include curbing the synthesis of histamine and encouraging its breakdown, as well as blocking phospholipase A2 to prevent production of arachidonic acid.6
However, complications have been associated with long-term use of topical corticosteroids, such as elevated IOP, cataract development and the exacerbation of existing viral or fungal infection.16 To address these complications in dry eye patients, drug manufacturers have developed loteprednol, the first broad-spectrum, anti-inflammatory topical ester corticosteroid that combines the benefits of a steroid — rapid action, site-specific activity, and less burning and stinging — with increased safety for long-term use. Drug companies have modified an existing molecule (prednisolone), replacing the portions that caused adverse effects.
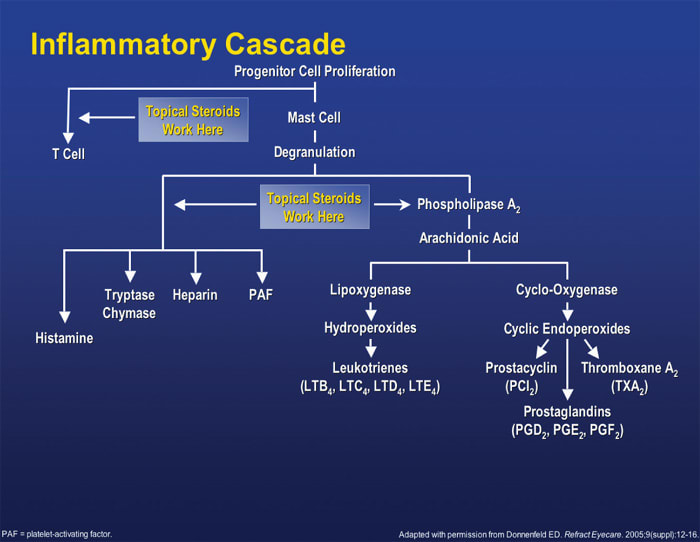
Topical corticosteroids interrupt the inflammatory cascade at key, early stages of the disease, limiting production of inflammatory precursor proteins at a nuclear level and controlling the increase of mast cells and lymphocytes at the cellular level.
Loteprednol etabonate
One of the advantages of loteprednol is that it treats all ocular surface inflammation associated with dry eye. Its highly lipophilic nature penetrates cells better than other corticosteroids. The glycerin in the drug penetrates cells neutrally. Plus, loteprednol specifically targets T-lymphocytes, which are found in high concentrations on the ocular surface in patients with dry eye.
Compared to dexamethasone, loteprednol has a lipophilic index that's 10 times higher and a binding affinity to steroid receptors that's 4.3 times greater.17,18 Unlike other corticosteroids, loteprednol becomes active only when it binds to a receptor,19 so less active drug is present that could increase the risk for elevated IOP or cataract development.19–21
Additionally, loteprednol resolves signs and symptoms of inflammation quickly. By reducing inflammation, it prevents further ocular surface damage, giving the surface a chance to repair itself. One study reported that patients treated with loteprednol showed improved central corneal staining and surface regularity at 2 weeks.22 What's more, investigators found clinically insignificant IOP changes after 1 month and reported no signs of cataract. So loteprednol is considered the safest topical corticosteroid.3
Loteprednol-cyclosporine combination
Given the unique advantages of loteprednol and cyclosporine, many eyecare practitioners use them in combination as a highly effective dry eye treatment. Loteprednol targets T-cells, whereas cyclosporine prevents T-cell recruitment, so fewer cytokines come to the ocular surface. Loteprednol works quickly, while cyclosporine may take 3 to 4 weeks to begin working. Used together, these agents complement one another, providing fast relief and long-term safety. I've never seen a cataract, secondary infection or other complication develop in patients after 3 years of using the drugs in combination.
For most dry eye cases, I prescribe loteprednol four times a day for 2 weeks, then lower the dosage to twice a day — during which time I add cyclosporine twice a day. Starting with loteprednol provides patients fast relief from the irritation, redness and burning associated with dry eye for a few weeks before they begin the cyclosporine. In my experience, this strategy has helped reduce burning and stinging upon instillation of the cyclosporine from 1 in 5 patients to nearly zero, so patients are much more likely to continue using it.
The effects from this combination not only resolve dry eye inflammation, they also give patients satisfaction and relief, often after suffering many years with discomfort.
Powerful synergy
Because our knowledge of dry eye has expanded over the years, we can offer more effective treatments to our patients. Combination therapy with loteprednol and cyclosporine has become the dry eye treatment of choice for many eyecare practitioners who have seen the powerful effect of this regimen. It provides fast and effective relief for our patients. Further studies examining combination therapy are under way, which may broaden our knowledge of dry eye further and demonstrate new ways for us to treat our patients. OM
| Dr. Karpecki specializes in cornea/external disease and research at the Cincinnati Eye Institute. He is chair of the Refractive Surgery Advisory Committee to the American Optometric Association and president of the Optometric Council on Refractive Technology. |
| References |
|---|
|