


vision therapy PART 1
Integrate Vision Therapy into Your Practice
Studies point to a large, unmet demand for vision therapy in the United States. In the first installment of this two-part series, the author discusses this opportunity and describes the VT evaluation, coding and the consultation.
BARRY TANNEN, O.D., F.C.O.V.D., F.A.A.O., Hamilton Square, N.J.
The American Optometric Association (AOA) defines vision therapy as: "… a sequence of activities individually prescribed and monitored by the doctor to develop efficient visual skills and processing. It is prescribed after a comprehensive eye examination has been performed and has indicated that vision therapy is an appropriate treatment option. The vision therapy program is based on the results of standardized tests, the needs of the patient and the patient's signs and symptoms. The use of lenses, prisms, filters, occluders, specialized instruments and computer programs is an integral part of vision therapy." (For more information, go to www.aoa.org/x5411.xml.)
Studies vary, but it's generally accepted that 10% to 20% of the general U.S. population has symptomatic binocular or accommodative vision problems. This means that anywhere from 300,000 to 600,000 people in the United States may be in need of vision therapy (VT).

Dr. Tannen works with a patient on vectogram training, which improves vergence ranges.
In reality, however, only a small fraction of the people who could benefit from VT actually will receive it.
I believe this is due to a lack of education and understanding among the public and various health-care professionals. Teachers often aren't trained to recognize how vision problems can affect a student in the classroom; pediatricians usually only screen for reduced visual acuity; and some optometrists and ophthalmologists are either biased against VT (due to lack of familiarity with current therapeutic regimens and/or the recent scientific literature that supports the efficacy of VT), or are undertrained in the detection and proper referral of patients who have binocular or accommodative disorders. This, in my opinion, has perpetuated a shortage of practitioners who specialize in VT.
While it's difficult to know for certain how many O.D.s offer office-based VT, about 1,600 optometrists are fellows or associates in the College of Optometrists in Vision Development, the main certifying body for VT specialists. This fact points to a potentially large unmet demand for the services that only VT-trained optometrists can perform.
In part one of this two-part article, I will define this specialty by acquainting you with the VT evaluation, coding for VT and VT consultation.
The Vision Therapy Evaluation
The Vision Therapy Evaluation (VTE) uses standardized optometric tests that stress the visual system to determine how it might be compromised during visual tasks, such as reading and computer work.
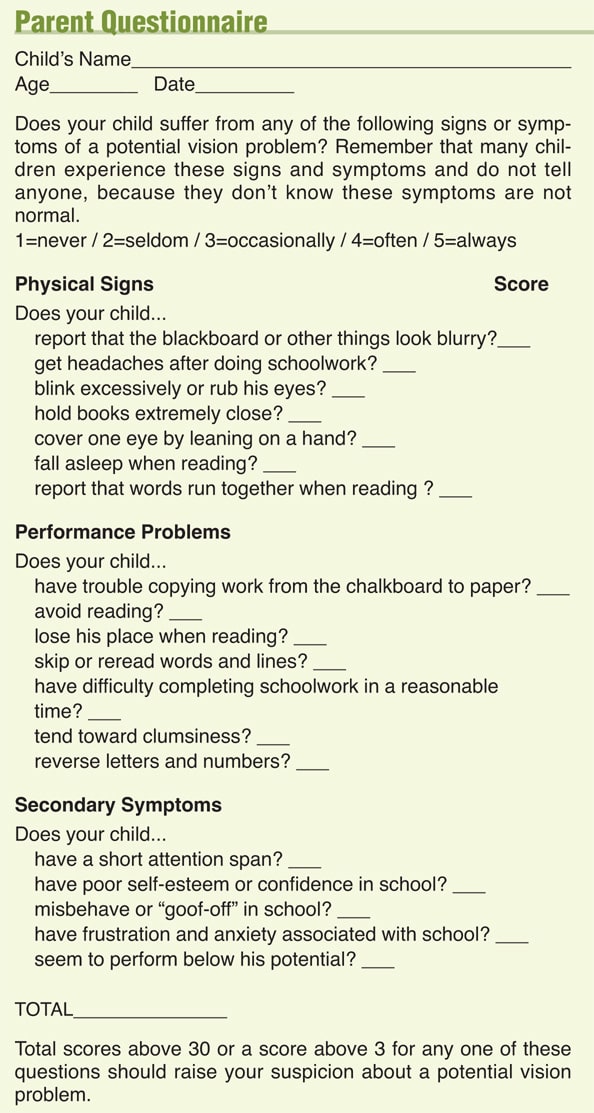
To aid in the acceptance of my recommendation for a VTE, I've developed a symptoms checklist that helps you identify the patients who most likely will require a VTE (see "Parent Questionnaire," page 68).
The list of tests that I may perform at a VTE, depending on the specific patient's age and symptoms, include:
■ Nine tests for binocular/accommodative disorders. These include the cover test (distance and near); nearpoint of convergence; phoria and vergence ranges (distance and near); accommodative convergence to accommodation (AC/A) ratio (gradient method); negative and positive relative accommodation (NRA/PRA); accommodative amplitude; accommodative facility test; vergence facility test and stereoacuity.
■ Eye movement testing. This includes my observation of the integrity and quality of pursuit and saccades; Developmental Eye Movement (DEM) or King-Devick tests, which measures the speed and accuracy of saccadic eye movements using a verbal test format; and the Visagraph Eye-Movement Recording System test, which evaluates the efficiency of the patient's reading eye movements.
■ Visual performance/binocular posture tests. This includes the Keystone Visual-Skills Test, which determines fusion, phoria and binocular posture in a stereoscope; the Cheiroscopic tracing and Van Orden Star tests, which determine patient's binocular posture and stability in free space using a unilateral (cheiroscopic tracing) or bimanual writing test (Van Orden Star); and monocular estimation method (MEM) retinoscopy, which objectively estimates the patient's accommodative response at near.
If I suspect a learning-related vision problem, I might also recommend a Visual Perceptual Evaluation (VPE) in addition to the VTE.
An example of a patient who might need a VPE: a child who reverses letters or words more often than the rest of his fellow classmates.
The VPE is a series of standardized tests that look at such skills as visual discrimination, visual memory, visual motor integration and letter/number reversal tendency, among others.
While full explanations of these individual tests is beyond the scope of this article, certain organizations, lectures, seminars and books can provide you with further education on this exciting specialty area.
Some examples: The College of Optometrists in Vision Development (www.covd.org), The Optometric Extension Program Foundation (www.oep. org) and the American Academy of Optometry (Binocular Vision, Perception and Pediatric Section) (www.aaopt.org).
An overview of coding for VTE
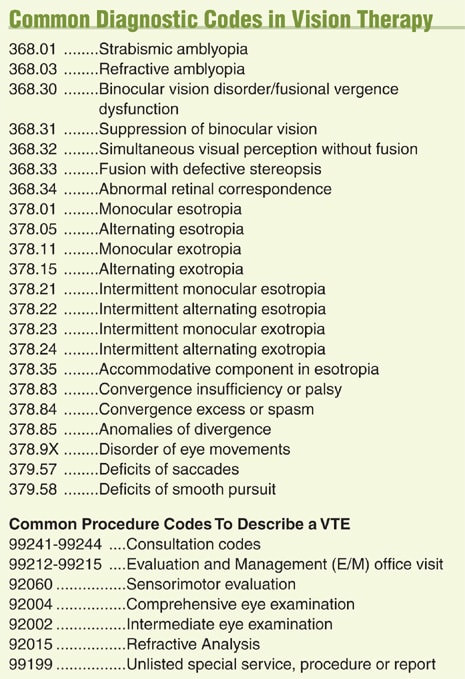
You can use the ICDM-9 diagnostic codes and the CPT codes to describe a VTE (see "Common Diagnostic Codes in Vision Therapy," page 86). For diagnostic codes, if possible, don't list the refractive status or an accommodative disorder as the first diagnosis, or most medical health insurance companies will likely reject the claim as "routine vision care."
Also, recognize that some parts of the evaluation may defy traditional medical CPT codes.
For example, an optometric visual perception evaluation isn't properly described by any CPT code in my opinion. Therefore, you can use the unlisted code (99199) and have the patient sign an Advanced Beneficiary Notice (ABN) that states he's aware that your evaluation isn't covered by his health insurance.
The Vision Therapy Consultation
I prefer to have the patient (or, more commonly, the patient's parents) return separately from the VTE for a VT consultation.
I typically schedule 40 minutes for this appointment, as it includes the presentation of the written report, my recommendations and the time spent with our VT coordinator to review fees and scheduling (if VT is recommended). In our practice, the VT therapy coordinator is an accomplished vision therapist who has the additional responsibility of presenting fees to the patient, scheduling the patient for VT and contacting insurance companies to find out if they can cover any part of the VT program.

Dr. Tannen works with a patient on aperture rule, which helps train accommodation and convergence at the same time.
I find it especially helpful that both parents be present if the patient is a child. This is because it's often very difficult for one parent to adequately explain the nature of the vision disorder and treatment to the other.
The purpose of the parent consultation is to:
1. Explain the difference between having good "visual acuity" and having a "vision problem." To make this point, I explain that the 20/20 visual acuity test never reveals why the child gets headaches after reading, sees double at near, loses his place when reading, etc. These are symptoms of a vision problem, not a 20/20 problem.
2. Demonstrate the effects of a vision problem. For example, to show what it might be like for a child to have diplopia from convergence insufficiency, I take two transparencies (the type used for overhead projectors) with the same paragraph printed on them. Against a blank white sheet of paper, I slightly misalign them to give the parents an idea of how disabling double vision can be.
3. Let parents know what vision therapy is and how it can help their child's vision problem. About 75% of the patients for whom I recommend vision therapy eventually accept the recommendation.
Example: Jenny is an 11-year old girl who I diagnosed with convergence insufficiency. Recently she's complained of headaches after 15 minutes of reading, intermittent double vision, excessive rubbing and blinking of her eyes and a general reduction in her interest for reading and doing her homework.
While demonstrating the effect of her double vision by using two transparencies, I said to her parents:
"Can you read this?"
Her mother shook her head "no."
"I think you can, try. You can read this paragraph, but you'd rather not. This is the case with Jenny. She can read with her vision problem, but it's very uncomfortable, and she doesn't want to do it for pleasure like she used to. With a VT program, we can restore her ability to read comfortably and efficiently."
Jenny's parent's next question was when we could get started.
In the second installment of this series, I will cover fee presentation (regardless of whether insurance covers VT), coding and billing for the VT sessions (as opposed to the diagnostic evaluation) and the VT patient agreement. I will also discuss the diagnostic and therapy equipment necessary to provide VT services, VT forms you can use for recording the results of VT, the VT report, office design for a VT room, how to train staff to become VT assistants, the success rates for VT in various conditions and a checklist for getting started. OM
| Dr. Tannen is in a private-group optometric practice in Hamilton Square, N.J., specializing in pediatric care, binocular vision disorders, vision therapy and learning-related vision problems. He is also an associate clinical professor of Optometry at the State University of New York College of Optometry, where he teaches the Vision Therapy course. E-mail him at BTannenOD@aol.com. |

|