


dry eye
DRY EYE One Treatment Does Not Fit All
To successfully treat dry eye, first determine the specific underlying cause(s).
WILLIAM TOWNSEND, O.D., Amarillo, Texas
Dry eye syndrome (DES) is one of the most challenging ocular conditions to treat because its symptoms of blurred vision, dryness, burning, stinging, grittiness, foreign-body sensation and increased light sensitivity do not signal one definitive underlying cause, and therefore one treatment. Therapy is also contingent on the quality and quantity of various components of each patient's tears.
Factors associated with dry eye
Researchers have discovered five strong associations with DES:► Advancing age. The rate of tear secretion and tear turnover decreases with advancing age.1
► Anticholinergic medications. These include tricyclic antidepressants, antihistamines and decongestants, isotretinoin-type drugs for acne treatment, opiate pain relievers, diuretics and some drugs commonly used to treat high-blood pressure.2
► Poor diet. Excessive ingestion of dietary fats, salt, cholesterol, alcohol, protein, caffeine and sucrose have been associated with, or suggested as causes of, tear dysfunction.3
► Heating/cooling systems. These devices reduce ambient moisture. Low environmental humidity plays a role in aqueous tear evaporation dynamics.4,5
► Hormonal changes. The duration of menopause and use of hormone replacement therapy (HRT) may increase the incidence of dry eye in post-menopausal women.6 Also, chronic androgen deficiency is associated with meibomian gland dysfunction (a form of lid disease) and dry eye.7,8
► Autoimmune disorders. Diabetes mellitus, rheumatoid arthritis, systemic lupus erythematosis, Human Immune Deficiency Virus (HIV), Stevens-Johnson syndrome, thyroid dysfunction and acne rosacea, among others, have been implicated in dry eye.9-15
► Contact lens use. Ocular problems induced by dry eye are associated with contact lens intolerance.16
► Cancer and bone marrow transplantation. Cancer survivors may experience dry eye due to systemic chemotherapy, radiation therapy or ocular graft vs. host disease as a complication of bone marrow transplantation.17
► Computer use. Sustained video display terminal operation and eye-fixation to a computer monitor, along with an associated decreased blink rate can cause eyestrain, eye fatigue, burning, irritation, redness, blurred vision and dry eye.17
► Refractive surgery. Procedures, such as LASIK, which sever corneal nerves interrupt the neural feedback loop from the eye to the brain and thus disrupt ocular surface tear dynamics, result in reduced tear production and ocular irritation.18
Diagnostic tools
Although dry eye is multifactorial in nature, there may be one prevalent causative factor in a patient's dry-eye condition. Once you've determined the factors associated with a patient's dry eye, evaluate the quality and quantity of his tears, so you can determine the most appropriate treatment regimen. The Diagnostic Methodology Subcommittee of the International Dry Eye Workshop (DEWS) — a group comprised of an international panel of experts in dry eye disease — recommends you use these six diagnostic tests.19

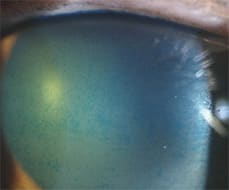
Lid wiper changes in a 73-year-old female with severe meibomian gland dysfunction and aqueous layer deficiency.
PHOTO BY CHAD BAKER
- Symptom questionnaires. The Diagnostic Methodology Subcommittee concluded that administering a structured questionnaire to dry-eye suspects provides a helpful screening opportunity. They cite 13 existing symptom questionnaires, among them: McMonnies, the Canada Dry Eye Epidemiology Study (CANDEES) and The Ocular Surface Disease Index (OSDI).17 The Subcommittee based the selection of these questionnaires on five criteria: used in randomized clinical trials; tested or used in epidemiologic studies; underwent some psychometric testing; availability and appropriateness for generic, non-disease-specific dry-eye populations.19 Use such questionnaires in conjunction with the patient's dry-eye status when determining treatment, the subcommittee says, as symptomatology is critical in making a dry-eye diagnosis.19 In particular, record the patient's worst and most bothersome symptoms, and the time of day in which they occur. Meibomian gland dysfunction tends to be most symptomatic early in the day in contrast with aqueous-layer deficiency, which tends to be more bothersome late in the day.
- Grade ocular surface staining. The Subcommittee recommends the use of fluorescein dye for corneal staining and lissa-mine green for conjunctival staining.19 These dyes offer a simple means of identifying ocular-surface changes. Use of a yellow barrier filter greatly enhances your view of fluorescein staining.19 Lissamine green is best visualized with reduced illumination. Practitioners currently employ three grading tests: the van Bijsterveld system, the National Eye Institute (NEI)/Industry Workshop system and the Oxford System.19 One grading system is not superior, according to the DEWS Diagnostic Methodology Subcommittee.19
- Tear film stability — tear film break-up time (TBUT). Practitioners generally evaluate TBUT shortly after the instillation of fluorescein or lissamine green staining. To enhance the visibility of the break-up of the fluorescent tear film, you can also use a yellow-barrier filter.19
- Non-anesthetized Schirmer test. This test determines whether the patient's accessory and main lacrimal glands can produce an aqueous layer when stimulated. The Subcommittee states that a reasonable cut-off for this test is less than 5mm of tear wetting on the strip in five minutes.19 If the mild irritation of the Schirmer's strip fails to elicit any tearing, the patient likely has poor tear production. I tape or glue the Schirmer strips to the patient's chart to determine a treatment plan.
- Measure Tear osmolarity. Many practitioners regard tear osmolarity as the key feature of ocular-surface dryness. Tear concentration values measured at greater than 316 milliosmolarity per kilogram (mOsm/kg) are likely to indicate dry eye.19
- Combination testing. Some practitioners have combined tests in patients who meet the dry-eye entry criteria, symptom or symptoms along with one or more positive test results of one of the aforementioned diagnostic tests.19 Check out the classification criteria of the American-European Consensus group to find the validated use of a combination of tests for dry-eye diagnosis.21
Practitioners have long used strips wetted with saline or drops to administer fluorescein dye and lissamine green, but delivering a consistent volume and concentration to the eye is difficult. My solution: I perform staining using syringes filled with sterile, non-preserved fluorescein or lissa-mine green that I obtain from a compounding pharmacist. The pharmacist tips these syringes with a microfilter to prevent contamination, and I've found they are a much more convenient and consistent means of instillation.

Sterile compounded lissamine green and fluorescein in syringes enhance the quality and convenience of dry-eye staining.
A TBUT of less than 10 seconds is considered unstable, although a TBUT as low as six seconds has also revealed dry eye. Because surface active agents, such as those found in preserved solutions, can markedly affect TBUT, it's preferable to wet fluorescein strips with a non-preserved saline.
Ophthalmic Research Associates developed the Ocular Protection Index (OPI), a non-invasive test that measures the relationship between TBUT and interblink intervals. Basically, the test measures TBUT and the inter-blink interval (IBI) in seconds. Divide the TBUT by the IBI to determine the OPI, which is the ratio between TBUT and IBI. If the tear film breaks up before the patient blinks, the OPI is <1. If the tear film remains intact through the entire period between blinks, the OPI is >1. Evaluation of the patterns of TBUT may also provide deeper insight into tear-film instability and the interaction of the tear film with the ocular surface in dry eye patients.
Unfortunately, this test is currently limited to "research" settings. The good news: OcuSense Inc., a San Diego-based company, received patent approval for an in-office device for evaluating tear-film osmolarity called the TearLab, currently in development (www.ocusense.com).
Another device worth mentioning: the Touch Tear MicroAssay System (Touch Scientific, Inc.) This in-office test evaluates tear-film lactoferrin levels. Lactoferrin is a tear protein that modulates the inflammatory response, controls cell growth and protects the eye against infection. Lactoferrin has been established as a dry-eye marker.20
Diagnosis
The DEWS Definition and Classification Subcommittee has determined two major classes of dry eye:
► Aqueous tear-deficient dry eye. This dry eye is the result of reduced lacrimal tear secretion and volume.22 This causes ocular surface epithelial cell hyperosmolarity and activates an inflammatory cascade that involves mitogen-activated protein (MAP) kinases and NF-kB (nuclear factor-kappa B) signaling pathways and the accumulation of inflammatory cytokines. This dry-eye form has two major subclasses: Sjogren's syndrome dry eye (SSDE) and non-Sjogren's syndrome dry eye (NSDE).22
Within the Sjogren's syndrome category are two classifications: primary Sjogren's syndrome, which is aqueous tear-deficient dry eye coupled with dry mouth; and secondary Sjogren's syndrome, which is a combination of the features of primary Sjogren's syndrome with an autoimmune connective disease, such as systemic lupus erythematosis.22
Within the non-Sjogren's syndrome category are: obstruction of the lacrimal gland ducts; primary lacrimal gland deficiencies, as seen in age-related dry eye; secondary lacrimal gland deficiencies, as seen in AIDS-related dry eye; reflex hyposecretion, as seen in some contact-lens wearers; and reflex motor block, which is associated with systemic drug use.22
► Evaporative dry eye. These patients have an exposed ocular surface, which causes major tear loss, though their lacrimal gland functions normally. Intrinsic disease and/or extrinsic exposure causes this form of dry eye.22 Intrinsic disease includes meibomian gland dysfunction, a low blink rate or a disorder of the lid aperture and lid/globe congruity (ocular surface drying).22 Extrinsic exposure includes contact lens-wear, exposed ocular-surface disease, destabilization of the tear film, loss of goblet cells and allergic conjunctivitis.22
Customize therapy
When dealing with either class of dry eye, treatment approach is generally determined by disease severity and usually consists of:
► Artificial tears. Over-the-counter (OTC) non-preserved artificial tears or tears that have alternative preservatives work to lubricate the ocular surface. Avoid prescribing benzalkonium chloride (BAK)-preserved artificial tears, as they have the potential to cause additional ocular-surface damage.23
Notice the ocular surface damage, secondary to the repeated application of a BAK-preserved artificial drop.
One study of 40 dry-eye patients showed that unpreserved artificial tears may lead to an objective improvement in corneal surface disease in dry-eye patients, while the preservation of tear substitutes with BAK may counteract this improvement.24 Hormonal imbalances, such as androgen deficiency or autoimmune disorders, may negatively affect lipid production and hence produce an unstable tear film. To address this problem, many oil-based artificial tears are also available on the market.
► Corticosteroid. Corticosteroids work to decrease inflammation — a main component of dry eye in many patients. One study compared topical lote-prednol etabonate (Lotemax, Bausch & Lomb) with a placebo in treating more than 50 keratoconjunctivitis sicca patients who had a delayed tear clearance. Results revealed that use of this corticosteroid four times a day may benefit patients with keratoconjunctivitis sicca that has a moderate inflammatory component.25
► Cyclosporine. 0.05% cyclosporine (Restasis, Allergan) inhibits the action of T-lymphocytes, reducing the inflammation on the ocular surface and restoring the tears. In turn, this may result in a reduction of symptoms. One trial found cyclosporine-A ophthalmic emulsions 0.05%, 0.1%, 0.2%, and 0.4% to be safe, well tolerated, decrease the effect of dry eye on vision-related functioning and significantly improve moderate-to-severe ocular signs and symptoms of DES.26
The concomitant use of corticosteroids or HP-guar-based lubricant eye drops may be beneficial. For instance, one study revealed that the use of topical loteprednol etabonate used q.i.d. may benefit patients who have keratoconjunctivitis sicca that has at least a moderate inflammatory component.27
Also, some practitioners have chosen to use a corticosteroid in conjunction with cyclosporine, as the corticosteroid decreases the inflammation and the cyclosporine sustains T-cell mediation, goblet cell density and increases tear production.28
► Omega-3 essential fatty acids. The Omega-3 acid supplementation of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) is currently used in prescription form in the management of high triglycerides. You can find omega fatty acids naturally in coldwater, fatty fish, such as salmon, or in flaxseed oil. Also, several companies offer Omega-3 supplements specifically designed to enhance eye health. Epidemiological studies have demonstrated lower odds of having dry-eye disease if one consumes a diet high in omega fatty acids.29
► Punctal occlusion. Because some dry-eye patients are only capable of producing marginal amounts of tears, you may want to consider punctal occlusion. To determine the success of this treatment, initially insert the largest possible temporary plug that mimics, as closely as possible, the occlusive characteristics of the non-dissolvable plug you feel is best for the patient. A number of manufacturers produce temporary collagen implants. These devices dissolve after three-to-five days. So, be sure that you or a staff member contacts the patient during this window to determine whether the plugs were beneficial, caused epiphoria or had no affect at all. Improvement warrants non-dissolvable plug implantation.
When selecting a non-dissolvable plug, weigh the lid and punctal configuration and ease of removal. Lid and punctal configuration determines patient response. In selecting a "capped" plug, carefully consider lid apposition. To profile the eyelids, use a biomicroscope at low magnification and swing the observation system to the side. If the lid and puncta are in normal apposition to the conjunctival surface, consider a domed, tapered, shaft-type plug. If, however, the patient has a "rolled" puncta that points toward, or comes in contact with, the bulbar conjunctiva, consider an intracanalicular device, as these are more difficult to remove.
Because many dry-eye symptoms are not the result of a specific underlying pathology, the days of randomly handing out drops are long behind us. While patient questioning and performing the aforementioned diagnostic tests can be a time-consuming and challenging process, doing so enables us to appropriately tailor our treatment regimen, so the patient can obtain relief and reclaim his quality of life — a reward well worth the time and effort. OM
References furnished upon request.

Dr. Townsend practices in multiple locations. He is a distinguished visiting clinician in Residence at the University of Houston College of Optometry and also serves as an adjunct faculty member there. |