


dry eye
Create a Dry-Eye Niche
Increase your bottom line by identifying dry eye in your current patients.
Scot Morris, O.D., F.A.A.O., and Trisha C. Rogers, O.D. Conifer, Colo.
A total of 13% of adults older than age 40 have dry eye, according to the Beaver Dam Eye Study. This translates into 17 2000 U.S. Census (the most recent million Americans, based on the U.S. Census Bureau's most recent (2006) population data. Further, the incidence of dry eye is much higher among contact-lens wearers (64%) than among those who wear glasses only (39%) or those who don't require vision correction (28%), according to findings from the 2005 Gallup Survey of Dry Eye Sufferers.
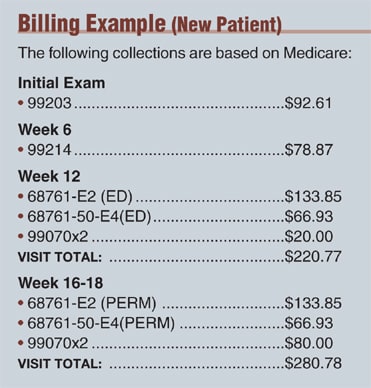
Essentially, if you're seeing the national average patient load of about 12 patients per day, based on the American Optometric Association's "2006 Caring for the Eyes of America: A Profile of the Optometric Profession" publication, you're seeing at least two dry-eye patients per day. A conservative estimate of the average collections per dry-eye patient is around $197.70. Annualized, that's about $102,485 per practitioner. (See "Billing Example"). That's a nice boost to your practice's bottom line.
The problem: Many optometrists are missing out on this increased income, as they falsely wait for their patients to complain of dry eye instead of becoming active in promoting their ability to diagnose and manage the condition. Realistically, patients rarely report dry eye until it's moderate to severe, and even then they may not tell you about it. The reasons for this:
► Many patients unfortunately view optometry as a spectacle- and contact-lens driven profession alone. In other words, they fail to see that we're also experts in the management of ocular conditions, such as dry eye. So, they present for prescription renewals but seek care for their ocular problems elsewhere.
► Many patients who present for an exam unrelated to an ocular condition may recognize our abilities as healthcare professionals, yet not realize the symptoms to which they've become accustomed are related to dry eye.
So, how can you identify dry eye in your current patients to improve their quality of life and your practice revenue? Through a very powerful form of internal marketing: patient education (See "External Marketing Tips"). Here are four effective methods:
1. Train your staff
Your staff is the face and voice of your practice. As a result, it's imperative you train them to become your ally in educating patients. Do this by conducting a series of training sessions on dry eye that detail common symptoms associated with the condition and the potential treatment options. These sessions will give them the knowledge they need to ask patients questions pertaining to dry eye during the medical-history taking, phone triage, etc.
Staff interaction with patients prior to your patient encounter makes patients consider issues they may otherwise not have, which will make them more likely to address these issues with you. This means you'll be able to help patients who may have ocular problems, while possibly boosting your practice revenue.
2. Use a questionnaire
Replace the out-of-date, tattered magazines in your reception room with an ocular surface disease (OSD) questionnaire. (Currently, the International Dry Eye Workshop [DEWS] cites 13 existing symptom questionnaires, including The Ocular Surface Disease Index). The appearance of the questionnaire not only elevates your status as a healthcare practitioner in the eyes of your current patients (now they know your expertise exceeds spectacle- and contact-lens prescriptions), but is a non-sales-pitch way of educating them that they, or someone they know, may have a condition that requires care, and you provide that care.
| External Marketing Tips To market your dry-eye niche externally, implement the following: ■ Annual Newsletter: This is a must have in your practice to make patients aware of your dry-eye skills and should include a special section designated to every niche you offer. ■ Direct Mail: Consider creating a direct-mail piece to every patient ages 35-65 (dry-eye patient demographic) in your practice. You may want to be even more specific, and narrow your mailings to your contact-lens patients to really get a great return on your investment. ■ Phone Message: Instead of on-hold music, have a customized phone message that includes your ability to diagnose and treat many eye-health issues, such as dry eye. This lets your current and prospective patients know that you're an astute practitioner in many fields of eye care. To be even more effective, you may want to look into having a message tailored to your practice's specialties. ■ Referrals: Motivate your current patients to provide new patient referrals by developing a new patient referral program with movie tickets, etc. ■ Write a follow-up letter: Always write a follow-up education letter and/or thank-you note to your patient. This not only acts as a nice, personal touch to show you care — instilling patient loyalty — but it also works to reinforce compliance to your prescribed treatment. |
Another internal marketing item for your reception room: In-office brochures. Brochures on dry-eye disease, among other ocular conditions, also serve to both educate the patient and dispel his preconceived notions about your abilities.
3. Inquire about dry-eye
Once the patient is in your exam chair, immediately ask him whether he's filled out the OSD questionnaire or whether he has any questions about any of the brochures he's seen in your reception area. Remember: Just because a patient's record indicates his visit is for an annual eye exam or prescription problem, doesn't mean he's not dealing with other ocular issues. You won't know unless you ask. Again, some patients may not realize that the symptoms to which they've become accustomed are related to dry-eye disease — a serious condition that warrants practitioner intervention.
If, indeed, the patient has filled out the dry-eye questionnaire, carefully read it over, so you can determine whether he may have the condition. While evaluating the questionnaire, ask any necessary follow-up questions, and invite the patient to ask you any related questions. Doing these things sends a message to the patient that dry eye is a serious ailment, regardless of whether he has it. In knowing this, the patient will likely refer friends or family members to you who have complained of dry-eye symptoms, such as foreign-body sensation.
In addition, if the patient doesn't have the condition, your interaction will likely make him vigilant about identifying these symptoms and immediately presenting to you in the future. This is because you've taken the time to discuss the condition, which has sent the message to the patient that it's serious. Also, your internal marketing in the reception room as well as your display of knowledge on the condition in the exam room has shown him you're able to treat and manage dry eye.
If the questionnaire indicates a possible diagnosis of dry eye, complete the intended exam (the reason the patient's presented), and schedule the patient for a dry-eye evaluation exam. Explain to the patient that dry eye is a chronic, yet manageable condition, but that there is a protocol to effective diagnosis and management. Further explain that as a result of this protocol, you may not be able to identify the cause and alleviate the symptoms in one visit. This conversation subtly establishes that management may involve multiple medical visits, in addition to the patient's annual eye exam.
4. Demonstrate your skills
At the patient's dry-eye evaluation, explain the different types of dry eye (aqueous tear-deficient and evaporative) and their causes, such as contact-lens use and refractive surgery. Also, describe the testing you'll be conducting, such as ocular surface staining and the purpose for each test. Finally, explain the treatment options available. (See "The Exam," below.)
For example, when assessing the lipid layer, you may develop a script similar to the following:
… Next, I'm going to check the outer oil layer of your tear film. This oil layer functions to prevent the underlying water layer from evaporating so quickly. Every time you blink, the muscles in your eyelid push on the small glands on the inside of your eyelid and push oil out of small holes at the margin of your eyelids. This oil is then deposited on the tear film and spreads across the surface of the eye every time you blink. I'm going to gently push on these glands to evaluate the quantity and quality of this oil layer. Problems in either the quality or quantity may lead to lipid (oil)-based dry eye — a form of evaporative dry eye, which often leads to symptoms, such as your eye feeling as if it's "stuck shut" in the morning. If this layer isn't normal, then the underlying water layer may also evaporate too quickly and lead to other forms of dry eye as well.
After assessing the lipid layer:
| The Exam The first step in any medical visit: Establish medical necessity by documenting a medical chief complaint. Then, document the patient's medical history, exam findings, patient education and complete diagnosis and treatment plan. All medical patients fall into one category based on patient status in your practice and the level of history taking, exam components and medical decision-making that you documented: • New Patients (99201-99205) • Established Patients (99211-99215) If you're not familiar with the criteria for each of the codes mentioned, familiarize yourself with them before initiating submission for reimbursement. Also be sure to use the correct procedure, and supply codes when appropriate. • Procedure codes: 68761 (punctal closure by implant) • Supply codes: Medicare no longer reimburses "A" codes for silicone plugs. Something else to keep in mind: Many third-party insurance carriers are following Medicare's decision to discontinue reimbursement for the materials (plugs) last year and are denying 99070 (miscellaneous supply code) at this point. But, it is still variable, so continue to bill the 99070 code. If Medicare denies your claim, you can choose to (preferably) bill the patient, although this is contingent on whether you had him sign a financial responsibility waiver. Another option: You can write it off. |
The oil is supposed to have the consistency of olive oil. Yours is a little thicker than normal. It has the consistency of butter, and I'm not able to push any out of the glands without using a lot of pressure. To treat this form of dry eye, I'm going to have you use hot compresses, which will help to "melt" the oil. I'm also going to prescribe artificial tears specifically designed to help replace the oil you're not making on your own. Finally, I'm going to start you on an omega-3 and omega-6 fatty-acid blend supplement, which will help your body to make more of its own normal oil.
This entire conversation takes about two minutes and conveys a great deal more information than "your eyes are dry." When you demonstrate your skills as an astute clinician by explaining dry-eye forms, testing and the purpose of treatments, you further demonstrate your skills as an astute clinician. This in turn makes your current patients who present for dry-eye evaluations stick with you as their dry-eye specialist, and refer others for your care.
Everything you treat in your practice is related to how you market yourself. By implementing patient education — a very strong form of internal marketing — you'll be able to sleuth out dry-eye disease in every patient who presents with clinical signs or symptoms. This will not only vastly improve your patient's quality of life (making them fiercely loyal, which will lead to referrals), but your bottom line as well. OM

| Dr Morris is the director of Eye Consultants of Colorado, LLC, and Morris Education & Consulting Associates. He is a member of the American Optometric Association and is a Fellow of the American Academy of Optometry. E-mail him at smorris@eye consultantsofco.com. |

| Dr. Rogers is an associate optometrist at Eye Consultants of Colorado, LLC. E-mail her at trogers@ eyeconsult antsofco.com. |