


Choosing Phakic IOLs Instead of LASIK
When LASIK isn't the answer, these lenses may offer an alternative for patients with myopia and astigmatism.
LASIK has helped many patients obtain the surgical vision correction they desire, but it has its limitations. When LASIK isn't the right choice for our patients, lens-based procedures are an attractive option.
To treat high myopia, we can choose from two FDA-approved phakic IOLs, both of which have a different set of parameters, advantages and associated complications. Several of the phakic IOLs in clinical trials make the lenses an increasingly valuable treatment option.
Saying ‘No’ to LASIK
LASIK is a prolific procedure — the gold standard by which many patients judge all ophthalmic surgery outcomes today. Nevertheless, when I see patients, often I'm looking for reasons why they shouldn't have LASIK. Patients expect excellent results, so I advocate LASIK only if it will meet expectations better than any other option.
Consider these limitations of LASIK:
■ High myopia: In our practice, we don't recommend LASIK for patients with myopia above –10.00D, although the standard may reach –9.00D in about a year.
■ Corneal thickness: Keratectasia is a risk post-LASIK. We don't know exactly what causes it, but we know that leaving a residual corneal bed less than 250 microns after LASIK is risky. Most surgery centers leave about 300 microns.
■ Keratometry: We rely on a patient's keratometry reading to determine whether LASIK is appropriate. We don't want to make the cornea too prolate or too oblate.
■ Hyperopia: To me, hyperopic LASIK is the biggest challenge. The general limits are +0.50D to +6.00D, and the standard right now for most surgery centers is about 4.50D of hyperopia.
■ Regression, predictability and IOP: All of these factors present challenges to using LASIK. In particular, hyperopic LASIK regression may occur within the first 2 to 3 years, thus necessitating an enhancement. Moreover, when patients have surgery on the cornea, we change the ability to accurately measure IOP. We must be especially careful when measuring IOP in patients with a family history of glaucoma.
| Phakic IOLs offer a natural and substantial amplitude of accommodation and excellent vision quality. |
■ Topography: When we see topography issues — for example, some inferior steepening or an aberrant type, such as pellucid or forme fruste keratoconus — we have to ask if LASIK is worth the risk.
When LASIK isn't the best option, epi-LASIK is a possibility, as are, of course, spectacles or contact lenses. And we can offer another robust surgical option to patients with high myopia: phakic IOLs.
Phakic IOL advantages
For correction of high myopia, phakic IOLs offer several advantages over LASIK:
■ Range of correction: We can use phakic IOLs to treat a myriad of myopic prescriptions. We can't do LASIK on a patient with –15.00D, but we can use a phakic IOL because of its range of correction.
■ Removability: We can't undo LASIK, but we can remove an IOL. It gives me peace of mind, especially with higher corrections, that we can remove the IOL if there's any issue.
■ Stability: These lenses are shown to be stable over time.1
■ Common procedure: IOL implantation entails making a small corneal incision — something every cataract surgeon has been doing for 30 years. So this isn't a new procedure.
Finally, phakic IOLs offer a natural and substantial amplitude of accommodation and excellent vision quality. Two phakic IOLs are approved by the FDA. The anterior-chamber Verisyse (Advanced Medical Optics) and the posterior-chamber Visian ICL (STAAR Surgical Co.).
| Vision Correction With Toric IOLs |
|---|
| If a patient doesn't have problematic cataracts, why remove the crystalline lens? To improve vision. When astigmatic patients over 40 want to see better without their eyeglasses, stop using readers or avoid getting bifocals, LASIK is one option. But when a patient has more than 3 or 4 diopters of hyperopia, LASIK is never my first choice. My first choice is to remove the lens and replace it with a toric IOL. Removing the lens may improve vision in the long and short term. The IOL can deliver excellent vision, and we're removing the lens that's aging and acquiring spherical aberration. Two toric IOLs are available for patients with astigmatism. The Staar Toric IOL (Staar Surgical Co.) has a silicone toric plate haptic design with scored markings 180° apart at the haptic edges. The lenses are available in 2.00D and 3.50D, which can correct 1.40D and 2.30D of astigmatism, respectively. The AcrySof Toric IOL uses the same platform as the AcrySof Natural Single-Piece IOL, with etched marks on the peripheral aspect of the optic. The lens is available in 1.50D, 2.25D and 3.00D. |
Verisyse iris-fixated phakic IOL
The first phakic IOL approved by the FDA, the Verisyse, has parameters of –5.00D to about –20.00D, providing an excellent opportunity to get patients out of contact lenses or eyeglasses.
The Verisyse is made of rigid polymethylmethacrylate (PMMA) material. Optically, it's very clear, but the rigidity means the IOL isn't very forgiving from a surgical standpoint, because it requires a 6-mm incision. Still, the Verisyse continues to be a viable option today.
Like all phakic IOLs, the Verisyse has a wider range of correction than LASIK, and it doesn't change the cornea as LASIK does. Also, it has a larger optic zone than LASIK and one size fits all, so surgeons don't have to worry about ordering the right size.
But the big advantage of an iris-fixated phakic IOL is that surgeons can see where they're placing the lens. This is critical when we're talking about centering the IOL over the pupil and enclavating the lens into the iris.
Another advantage of the Verisyse and other phakic IOLs is that you can couple the implantation with other surgeries, known as bioptics. For example, to treat a patient with myopia of –10.00D and 3.00D of astigmatism, we can treat the myopia with the IOL and correct the astigmatism with LASIK or reduce it with a limbal relaxing incision. I usually tell these patients, "We'll deal with the astigmatism after the surgery." It works out well because the surgeon may induce some astigmatism during IOL implantation.
According to the FDA, several complications are associated with the Verisyse IOL, including increased risk of secondary glaucoma related to angle closure, glare and halos, low-grade inflammation, iris deformation and intraocular risks.2
And like all IOLs, the Verisyse can result in a reduction in the endothelial cell count. Before using a phakic IOL, we count the endothelial cells, check the patient's age and calculate an endothelial cell loss of 5% to 10% per year. We determine if the patient will have enough endothelial cells to avoid Fuchs' dystrophy. Patients with Fuchs' or a low endothelial cell count aren't candidates for phakic IOLs.
Visian posterior-chamber phakic ICL
The other FDA-approved phakic IOL, the Visian, is implanted in the posterior chamber. The rectangular lens is made of a proprietary material called "collamer," a collagen copolymer, giving the Visian the name "implanted collamer lens" or "ICL." This material attracts a substance in the aqueous called fibronectin, which coats the lens and reduces white cell adhesion. The lens is foldable, has a highly elastic nature and offers protection against UV rays.
According to FDA guidelines for the Visian lens, candidates are greater than –3.00D to –20.00D with an anterior chamber depth above 3.0 mm. The lens's practical range is about –16.50D to 17.00D. The cylinder custom power goes to 6.00D at any axis, 10.0 mm to 11.5 mm and 7.5 mm to 8.0 mm wide.3
Like the Verisyse, the Visian is limited by the anterior chamber depth. The Verisyse requires greater than 3.2 mm, while the Visian requires 3.0 mm. This is further complicated by the characteristically shallow anterior chambers of hyperopes and the need to stabilize the prescription. These factors make hyperopes a challenge. The Visian is implanted through a 2.8 mm to 3.0 mm incision to sit in the ciliary sulcus.
Like any IOL procedure, Visian insertion is familiar to cataract surgeons. The lens sits close to the nodal point and thus provides the best optical quality, and the incision is much smaller than that used for the Verisyse lens. The Visian offers some additional advantages over LASIK, such as fewer long-term complications with ICL power calculations.
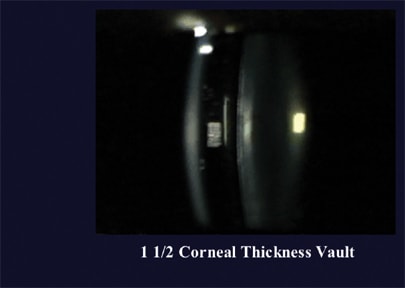
The slit lamp shows the front and back of the cornea. Based on this reference size, we can estimate the size of the vault (for example, the vault thickness may be 10% of the cornea's diameter).
Visian comanagement
When we comanage patients with the Visian lens, we must be mindful of both preoperative and postoperative considerations. For example, I carefully check vision to ensure that patients aren't developing cataracts.
In addition, as part of the candidate selection process, we need to check the vault. Using the slit lamp, we see the cornea's overall thickness. With this reference point of 1, we can evaluate the vault space. It should always be at least 10% of the corneal thickness. If the vault is less than 10%, then I send the patient back to the surgery center for evaluation. The surgeon has to measure limbus to limbus to ensure the lens is long enough to bow away from the anterior surface to the left.
Postoperative care is routine. Patients typically use moxifloxacin (Vigamox, Alcon) and prednisolone acetate for a week.
I monitor patients for complications, such as discomfort from the incision. Other possible complications include angle-closure glaucoma, pigment dispersion, anomalous ciliary anatomy, intraocular risks and lens opacities.
This final risk worries patients. In a clinical trial, the incidence of early subcapsular opacities was 1.7% (9 total).4 Researchers saw seven of these cases by the first week after surgery; eight were asymptomatic, and one occurred due to the use of a miotic with preservative irrigated into the anterior chamber during surgery. Late opacities (first seen at or after 12 months post-surgery) occurred in 0.6% of cases (3 total). Two cases required ICL removal: one for poor lens placement and the other was the case in which a miotic was used.
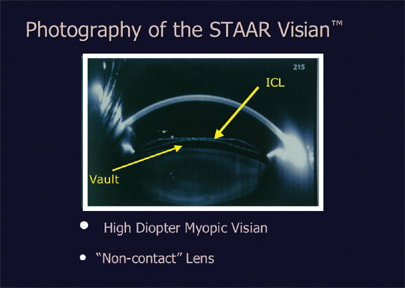
This ultrasound biomicroscope image shows the cornea and the myopic ICL (thicker on the edges and thinner in the center). The vault is clearly visible.
The surgeon can't see where this lens is placed because it sits behind the iris. In a hyperopic case, this was exemplified by the difference in uncorrected vision when the eyes were dilated and not dilated. Dilated, this patient was 20/15, however undilated, the patient was –2.50 D and his distance vision was extremely blurry. An ultrasound biomicroscope revealed that the lens sat somewhere on the ciliary body and changed shape when the ciliary body was accommodating or relaxing.
Both the Verisyse and the Visian are undergoing further development, and each incarnation of the lenses has carried lower risks. Among our treatment options for vision correction, phakic IOLs continue to expand their utility and value. OM
Marc Bloomenstein, O.D., F.A.A.O., is director of optometric services at the Schwartz Laser Eye Center in Scottsdale, Ariz. He's a founding member of the Optometric Council on Refractive Technology and president of the American Optometric Charitable Foundation.
| References |
|---|
|