


drugs
The Prescribing Perplexity
Here's our view on what to prescribe when faced with varying inflammatory ocular anomalies.
RANDALL THOMAS, O.D. M.P.H., F.A.A.O., Concord, N. C. AND RON MELTON, O.D., F.A.A.O., Charlotte, N. C.
When a patient presents with an ocular condition that has an inflammatory element, choosing the correct therapy can be challenging. This is because it's not always clear whether a bacterial pathogen is contributing to the inflammatory expression. The question then follows: "How do I know when to use a pure antibiotic, a pure corticosteroid or a combination antibiotic/corticosteroid product?" (See "Prescribing Pearls," below.)
| Prescribing Pearls |
|---|
| When treating with a combination drug, an antibiotic, or a pure corticosteroid, we encourage frequent initial dosing for one to three days before reducing the dosing frequency. We've discovered that this maximally enhances a therapeutic cure and the patient's comfort. Few conditions exist in which optimum therapy is q.i.d. for one week. Because most eye drop formulations are ophthalmic suspensions, we instruct patients to shake them well prior to each instillation. Many combination products are also available in ointment form. Such ointments can be particularly useful in treating allergic/inflammatory forms of eyelid disease, such as anterior blepharitis and contact/eczematoid blepharodermatitis. |
Here's our perspective:
Pure antibiotics
We rarely prescribe a pure antibiotic because patients rarely present to our practices displaying bacterial eye infections. Nevertheless, we've found success in using this drug class when faced with the following conditions:
► Evident mucopurulent discharge with mild inflammation. If the patient presents with evident mucopurulent discharge — the ultimate diagnostic marker for bacterial infection — and the eye is only mildly inflamed, we typically prescribe a pure antibiotic (aminoglycoside or fluoroquinolone) every q2h for two days, followed by every q4h for five more days. This is because we have found this therapy to be effective in eradicating the offending pathogen and therefore resolving the secondary inflammation.
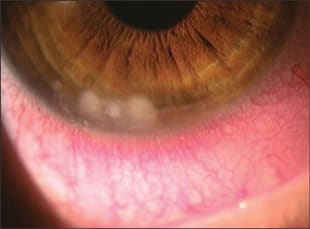
This contact lens wearer developed inferior conjunctival injection, which prompted her visit. Slit lamp examination revealed multiple Foci of leukocytic infiltration at the inferior cornea. We chose to treat this patient with a combination antibiotic steroid to quell the corneal and conjunctival inflammation and prevent any infiltration from opportunistic pathogens.
► Pronounced mucopurulent discharge in a markedly inflamed eye. In this case, we typically prescribe intensive antibiosis (aminoglycoside or fluoroquinolone) — meaning every hour or two for a couple of days — because we want to aggressively eradicate the bacterial pathogen from the ocular surface.
If the patient reveals significant secondary inflammation at follow-up, though the bacterial infection appears under control, we typically prescribe a corticosteroid to quell the remaining inflammation.
► Bacterial conjunctivitis in children. For a case in which the conjunctiva is mildly injected, but there is evident mucopurulent discharge, we typically prescribe a pure macrolide antibiotic formulation that offers a dosage of one drop into the affected eye b.i.d. for two days; then q.d. for five more days. This is because we've found that this drug quickly and effectively kills the offending pathogen, while providing an easy-to-comply with dosing schedule for these patients.
► True, or probable, bacterial conjunctivitis. When a patient presents with mucopurulent discharge in the tear film and on the eyelashes and eyelids, we typically prescribe a pure antibiotic (aminoglycoside or fluroquinolone) intensively — meaning every hour for a couple of days. In addition, if there was a concurrent eyelid infection, we would consider prescribing an oral antibiotic to get enough antibiosis into the eyelid's blood vessel system. The dosage and duration of use of the oral antibiotic is contingent on our selection of a specific oral antibiotic.
Then, we would reassess the condition. Depending on its presentation at the follow-up visit, we would either continue or reduce the frequency of dosing of both the topical and oral antibiotic.
► Marked bacterial infection. In the rare cases in which patients present with raging mucopurulent discharge, we typically consider adding Polysporin ointment at bed time for four to five nights in addition to intensive antibiosis (aminoglycoside or fluoroquinolone) — again, every hour for a couple of days. This provides the patient with good, around-the-clock antibiosis.
► Inflammatory processes of the cornea. If a patient presents with phlyctenules; infiltrate; corneal abrasions, corneal foreign body removal; or removal of conjunctival concretions, we typically prescribe pure antibiotic prophylaxis (aminoglycoside or fluoroquinolone). This is because these conditions and circumstances compromise the health of the corneal epithelium, making it susceptible to opportunistic pathogen infiltration.
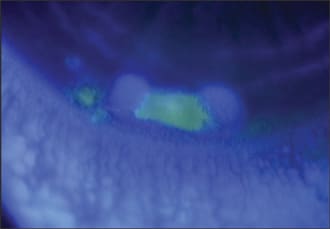
This contact lens wearer developed inferior conjunctival injection. Fluorescein dye revealed staining of the epithelium — a result of superficial compromise due to anterior stromal inflammation. We prescribed a combination drug, which nicely suppressed the primary inflammatory keratitis, while the antibiotic prevented any potential for opportunistic bacterial infection.
► Bacterial corneal infiltrate. Any infiltrate is potentially the beginning of an early expression of an infectious process; this, however, is exceedingly rare. Most all infiltrates are so-called "sterile" infiltrates, which are migratory, chemotactically attracted white blood cells (i.e., a cell-mediated immune response to a usually unknown noxious stimulus). You must understand that immune processes within the anterior stroma commonly cause some compromise to the overlying epithelium and that this can result in epithelial staining with fluorescein dye, although the staining defect is almost always smaller than the underlying stromal lesion.
A bacterial corneal infiltrate typically presents with a fluorescein-staining defect that tends to approximate the dimensions of the stromal defect. Other clinical features: a markedly injected eye, significant anterior chamber reaction and considerable pain. In this case, we would typically first instill a drop or two of a cycloplegic agent, such as 1% cyclopentolate, 5% homatropine, or 0.25% scopolamine, to help dampen the anterior uveal inflammation. Then, we would most certainly prescribe a pure antibiotic (an aminoglycoside or a fluoroquinolone) hourly for a day or two and then reassess the condition. Whether/when we decide to add a corticosteroid, we would expect the iridocyclitis to resolve quickly, along with the primary keratitis. (See "Contact Lens Patient With Recurrent Infiltrates," below.)
| A bacterial corneal infiltrate typically presents with a fluorescein-staining defect that tends to approximate the dimensions of the stromal defect. |
| Contact Lens Patient With Recurrent Infiltrates |
|---|
| If a patient presents with chronic, recurrent corneal infiltrates and reports sleeping in his contact lenses, we consider switching him to a daily wearing schedule. If the patient is already on this schedule, we encourage him to reduce his wearing time. In addition, we are sure to evaluate his tear film, as suboptimum precorneal tear film dysfunction and blepharitis place the patient at greater risk for bacterial pathogen infiltration. If blepharitis is present, we typically prescribe warm lid soaks via washcloth t.i.d. anywhere from one week to one month, depending on its clinical presentation, to loosen the thick secretions within the glands. Also, we have the patient immediately follow the warm soak with a lid massage, in which he expresses the meibomian glands. Then, we instruct patients to use a commercially available lid scrub, which we show them how to use in the exam room, to rid the lid of the debris leftover from lid soaks and lid massage. |
► Illusive diagnostic certainty of a corneal infiltrate. If a patient presents with a corneal infiltrate of which we're uncertain, though we have a gut feeling it may be infectious in nature, we typically prescribe either a pure aminoglycoside or fluoroquinolone hourly for a day or two. This is because the structural integrity of the corneal epithelium has broken down, exposing it to a bacterial infection. If the beginnings of a pathogen are present, we want to quickly eradicate it.
After this therapy, we reassess the corneal status. If the patient presents with "no major improvement," we consider inflammation to be the primary mechanism and switch the patient to a corticosteroid.
Pure corticosteroid
We typically prescribe a pure topical corticosteroid for all inflammatory conditions, in which we do not perceive a threat of opportunistic bacterial infection. These conditions include: episcleritis, uveitis, chemical/toxic conjunctivitis and other nonspecific ocular surface inflammatory conditions, such as blepharodermatitis.
Our rule of thumb: If the corneal epithelium is pristine and the lacrimal lake is clear, prescribe a pure corticosteroid. (See "Ocular Corticosteroids," below.)
| The Ocular Corticosteroids |
|---|
| • Dexamethasone 0.1% sodium phosphate (Maxidex, Alcon), (AK-Dex, Akorn) • Fluorometholone 0.1% alcohol (FML, Allergan), (Fluor-Op, Novartis) • Fluorometholone 0.1% acetate (Flarex, Alcon) • Fluorometholone 0.25% alcohol (FML Forte, Allergan) • *Loteprednol Etabonate 0.2% (Alrex, Bausch & Lomb), • *Loteprednol Etabonate 0.5% (Lotemax, Bausch & Lomb) • Medrysone alcohol 1% (HMS, Allergan) • Prednisolone 1% acetate (Omnipred, Alcon), (Pred Forte, Allergan) • Prednisolone 1% sodium phosphate (AK-Pred, Akorn), (Inflamase Forte, Novartis) • Prednisolone 0.125% sodium phosphate (AK-Pred, Akorn), (Inflamase Mild, Novartis), • Rimexolone 1% (Vexol, Alcon) * Ester-based |
One example of our therapeutic protocol:
► Blepharodermatitis. If a patient presents with blepharodermatitis, we typically prescribe 0.1% triamcinolone cream for use b.i.d. for four days; then just at bedtime for four more days, as this normally resolves the lid inflammation.
This corticosteroid comes in a 15g tube; however, it's not an ophthalmic formulation. In fact, the side of the tubes of both over-the-counter (OTC) hydrocortisone and prescription triamcinolone state, "not for ophthalmic use." This is not a practical problem, since we are not prescribing triamcinolone "in the eye." But, it's important to be aware of this statement because some/most patients (and pharmacists, too) may not realize this. Moreover, practitioners commonly inject triamcinolone acetonide into the eye for the treatment of uveitis and ocular inflammatory conditions unresponsive to topical corticosteroids.

This patient presented with classic phlyctenular keratoconjunctivitis — an immune response to staphylococcal exotoxins. We chose to prescribe a combination drug to suppress the inflammatory response, while eliminating the bacterial activity.
Because cases of episcleritis, uveitis and chemical/toxic conjunctivitis can present as mild, moderate or severe, their clinical presentation will dictate the amount and duration of the corticosteroid drop formulation.
Combination antibiotic-corticosteroid drug
The essential elements in selecting a combination antibiotic/corticosteroid drug are three-fold: First, ocular surface inflammation must be evident. Second, the eye must reveal evidence of either concurrent bacterial infection, or you must have a rational concern for opportunistic bacterial pathogen expression, which would then merit antimicrobial prophylaxis (i.e. a corneal epithelial defect). Third, the patient must not have herpes simplex, epithelial keratitis, fungal and/or acanthamoeba infections, as all are contraindications for this drug class. (Examples of alternative treatments for these patients: anti-herpetic drugs for patients with herpes simplex, neomycin for acanthamoeba infections and natamycin for a fungal infection.) (See "The Combination Antibiotic/Corticosteroid Drugs," below.)
| 0.1% triamcinolone cream can effectively treat blepharodermatitis. |
| The Combination Antibiotic/Corticosteroid Drugs |
|---|
| • Cortisporin ophthalmic ointment (neomycin, polymyxin B, bacitracin and 1% hydrocortisone) • Cortisporin ophthalmic suspension (neomycin, polymyxin B and 1% hydrocortisone) • Gentamicin 0.3% and prednisolone acetate 1.0% sterile ophthalmic suspension (Pred G, Allergan) • Gentamicin 0.3% and prednisolone acetate 0.6% sterile ophthalmic ointment (Pred G, Allergan) • Loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension (Zylet, Bausch & Lomb) • Neomycin and polymyxin B sulfate and dexamethasone 0.1% ophthalmic suspension (Maxitrol, Alcon) • Neomycin and polymyxin B sulfate and dexamethasone 0.1% ophthalmic ointment (Maxitrol, Alcon) • Sulfacetamide sodium 10% and prednisolone acetate ophthalmic ointment 0.2% (Blephamide, Allergan) • Sulfacetamide sodium 10% and prednisolone acetate ophthalmic suspension 0.2% (Blephamide, Allergan) • Tobramycin 0.3% and dexamethasone 0.1% sterile ophthalmic ointment (TobraDex, Alcon) • Tobramycin 0.3% and dexamethasone 0.1% sterile ophthalmic suspension (TobraDex, Alcon) |
We typically treat the following conditions with a combination drug:
► Bacterial conjunctivitis with significant conjunctival injection. We typically prescribe a combination drop for a bacterial conjunctivitis that has a significant amount of conjunctival injection, as the drug nicely eradicates the infectious component of the condition, while suppressing the inflammatory component. Typical dosing would be every q2h for two days and q.i.d. for four or five more days.
► A small corneal infiltrate near the limbus with sector injection. This presentation almost always represents a noninfectious condition. Further evidence of a noninfectious process is absent or minimal cellular response in the anterior chamber and an epithelial staining defect that is much smaller than the underlying anterior stromal infiltrate. Again, because we are dealing with the cornea, we typically prescribe a combination drop every q2h for two to three days, then q.i.d. for one week, in the rare event of bacterial etiology.
We hope this article assists you when faced with the choice of a pure antibiotic, pure corticosteroid or combination antibiotic/corticosteroid drug. We have practiced this way for more than 50 combined years without therapeutic misadventure, and we urge you to practice in such a manner so as to maximally enhance patient care. OM


|
Dr. Thomas practices at Cabarrus Eye Center in Concord, N.C., where he specializes in comprehensive eye care and glaucoma. Also, he is an internationally known speaker regarding ophthalmic medications. E-mail him at thomasepec@carolina.rr.com. Dr. Melton is currently in group practice in Charlotte, N.C. Also, he is an adjunct faculty member of the Pennsylvania College of Optometry at Salus University and the Indiana School of Optometry. E-mail him at meltonepec@aol.com. |