


cover feature
Ultra-Widefield Retinal Imaging: Is it Right for Your Practice?
The technology is changing patient care and how practitioners differentiate their practices.
VIRGINIA PICKLES
contributing editor
Not long ago, ultra-widefield retinal imaging using a scanning laser ophthalmoscope was slowly gaining acceptance in optometry and being touted for impressing patients with its "wow" factor. Numerous software enhancements and a new ultra-high resolution device have expanded the utility of this technology, so much so that a new set of questions arise: Where does ultra-widefield imaging, which provides a 200-degree view of the retina, fit in today's optometric practice (especially in light of current emphasis on medical eye care)? Are practices using this technology for screening, diagnosis or comanagement? What do patients think of it? And what sort of return on investment are they achieving? To find out, OM interviewed a cross-section of optometrists — from early adopters to new users — representing various regions, practice settings and sizes. Their insights appear on the following pages.
Facing the dilation dilemma
A retinal evaluation is a critical component of a comprehensive eye examination, yet some patients avoid having their pupils dilated for the traditional examination with a binocular indirect ophthalmoscope (BIO) because of the inconvenience. Other patients are unable to direct their gaze as required, perhaps because of age or disability, and despite their best efforts, their exams are less than optimal. Any of these scenarios can have dire consequences.
"Retinal disease, such as macular degeneration, is a leading cause of blindness," says Kim Castleberry, O.D., founder and CEO of Plano Eye Associates in Plano, Texas. "Moreover, many serious, even life-threatening conditions manifest in the retina."
Wayne J. Goldschneider, O.D., who, along with partners Dale Stein, O.D., and David Talbot, O.D., owns four independent optometric practices in Southern New Jersey, agrees. "In addition to uncovering peripheral retinal pathology, macular degeneration and glaucoma," he says, "retinal evaluation also can reveal changes due to systemic disease, such as diabetes and hypertension."
To ensure that all patients receive a comprehensive eye exam, including retinal evaluation, at every visit, the clinicians we interviewed now use ultra-widefield retinal imaging with the P200 scanning laser ophthalmoscope or the ultra-high resolution P200C (Optos, Marlborough, Mass.), which produce the Optomap retinal image. This nonmydriatic option captures an image of the retina in less than a second without any discomfort to the patient.

|
|
Because Optomap ultra-widefield images are high resolution, you can zoom-in on pathologies or suspected pathologies. Left is an Optomap widefield image of a classic horseshoe tear. Right, the tear from the same image is enlarged.
Dr. Goldschneider notes that while the Optomap screening does not replace a dilated exam in all situations, he estimates he now dilates 10% to 15% of his patients. "Before we started using Optomap, we were dilating most patients," he says.
Dr. Goldschneider explains: "When patients have symptoms of retinal pathology, such as retinal detachment, we use the Optomap as a guide and as a documenting tool, but we also dilate the patient to evaluate the retina. We also dilate our patients who have been diagnosed with glaucoma, macular degeneration, etc. In other words, when retinal or optic nerve disease is present or suspected, we always perform a dilated examination in addition to Optomap scans."
A thousand words
"If the adage ‘a picture is worth a thousand words’ is true, then an Optomap image is a thousand words," says David R. Frazee, O.D., a solo practitioner in Richardson, Texas. "Drawing and describing what you have seen using the BIO is never as accurate as a picture. Optomap images help me explain how the eye works, what pathology a patient has and its impact on his vision and treatment plan."
According to Gregg Ossip, O.D., CEO of Ossip Optometry with 16 offices in central Indiana, "The ability to instantly obtain retinal data without inconveniencing the patient time-wise is awesome. I truly appreciate being able to see the whole retina at once as opposed to trying to patch different views together. I like that I can manipulate the images and see the different layers of the retina." For example, says Dr. Ossip, by manipulating the different layers of the retina on the Optomap, he can "tell if a spot of pigmentation is a nevus or a malignant melanoma."
For Ryan L. Parker, O.D., a solo practitioner in Ardmore, Okla., being able to perform a thorough, efficient retinal examination is "huge." As he explains: "Our closest retina specialist is in Oklahoma City, which is 90 minutes away. We have two excellent ophthalmologists in town, but their focus is on cataract surgery. So if I don't perform a retinal evaluation, it probably won't be done routinely."

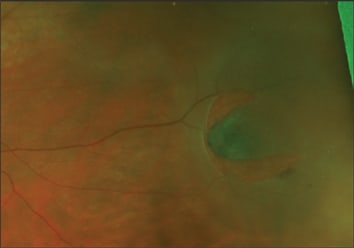
An Optomap retinal scan, taken by the P200C, shows a retinal detachment.
The practitioners we interviewed offer Optomap screening to all patients at every annual examination. "We offer wellness Optomap screenings to all wellness eye exam patients," Dr. Castleberry says. "We order medically necessary Optomap Plus for patients requiring special diagnostic testing for suspected or manifest eye disease, such as glaucoma, diabetes, diabetic background retinopathy, proliferative diabetic retinopathy, diabetic macular edema, clinically significant macular edema, posterior vitreous detachment, floaters, and epi-retinal membrane, to name a few."
| Screenings vs. Diagnosis: What's Covered? |
|---|
| Optomap retinal screening is an optional test offered to all patients in all the practices we contacted. Fees for screenings are not reimbursed by third-party payers. "I like this because I'm paid the day of service and don't have to submit associated claims," says Kim Castleberry, O.D. "Optomap screenings also lower my insurance cost profiles by shifting costs to the patient for imaging that I need, at the same time improving my quality reporting index. A better cost and quality index with insurance companies makes my practice more attractive to insurance companies and patients. I use a level III CPT code S9986 and bill an associated well-vision ICD code. "Optomap Plus medical exams are reimbursable by most third-party medical plans for reasonable and medically necessary care when the exam is to evaluate a medical eye problem," Dr. Castleberry continues. "Optomap Plus software supports CPT codes 92250 (fundus photography with interpretation and report), 92225 (extended ophthalmoscopy) and 92226 (extended ophthalmoscopy, subsequent), with an appropriate medical ICD diagnosis code." |
Screening efficiently
To facilitate Optomap screening and improve patient flow, Optos has revised its software — the P200 and the P200C are fee-per-scan devices — so that a fee is charged only when an image is opened. "Most of our patients provide an informed consent to have an Optomap screening test," Dr. Ossip says. "Previously, if they declined the screening initially and then chose to have it after speaking with the doctor, they had to return to the testing area, which interrupted patient flow. So we worked with Optos to find a solution. Now, we capture images of all patients in our pretest area, but billing occurs only if the doctor reviews an image. With this procedure, the doctor can discuss the benefits of the technology with the patient before the patient makes a decision (whether he wants to pay out-of-pocket for the assessment), and our patient flow is not interrupted."
Most of the doctors we interviewed follow the procedure Dr. Ossip outlined. They report acceptance rates from 75% to 90%.
According to Dr. Parker, who has a fairly large pediatric population, Optomap imaging is advantageous for children, as well. "Drops traumatize kids because they sting," he says. "Take eye drops out of the equation, and you'll make the experience a lot better for them."
What will you see?
The technology also impressed doctors who report finding a wide range of retinal anomalies with Optomap screening. Brian M. Dembo, O.D., who practices in Glenview, Ill., provides and example:
"The case that underscores the value of the Optomap for me is the 22-year-old asymptomatic man who was sitting in my chair only because he had broken his glasses," Dr. Dembo recalls. "He'd had a dilated examination by an ophthalmologist 18 months before seeing me. The Optomap picked up a lesion in the far peripheral retina that turned out to be a melanoma. I am convinced that even with dilation I would have missed it, because this is the type of patient who has difficulty keeping his eyes open. The technology not only saved his eye but potentially his life."
Vernon Prentice, O.D., who practices in Pembroke, Ontario, Canada, identified a metastatic carcinoma that computed tomography (CT) scanning, failed to show. "The Optomap showed the lesion, but when I first examined the eye with fundus biomicroscopy after this detection, I did not see the lesion. I had to go back to the Optomap to confirm that I had, in fact, seen it in the left eye. I found it possible to detect after a second look with fundus biomicroscopy, but I thought how easily it could have been missed without the Optomap." One of the most recent upgrades to the Optomap Plus examination software is the ResMax feature, a high-resolution enhancement for viewing the central pole. Using this feature, Dr. Castleberry determined that a 76-year-old patient's reduced visual acuity was secondary to vitreomacular traction-induced epiretinal membrane. "The dual laser technology allowed separation of the retinal layers so I could accurately diagnose, document and follow the patient's condition," Dr. Castleberry says.
These sight-saving, sometimes life-saving, diagnoses have convinced these doctors that offering ultra-widefield retinal imaging is the right thing to do. "You have no idea what you're missing until you start looking at images like these," Dr. Parker says. Before saying yes to the Optomap, however, these practitioners considered many factors, not the least of which involved finances.
ROI and beyond
No initial cash outlay is required for an Optomap retinal system. Optos charges a monthly fee based on the number of scans prepaid each month, says Dr. Parker. "As that number increases, the per-scan charge decreases," he says. Dr. Parker provides the following example financial example:
"In June, we performed 94 scans at a cost of $2,162, for which we charged $3,008, netting $846. In July, we performed 121 scans at a cost of $2,783, for which we charged $3,872, netting $1,089." (Note that fees charged to patients vary from practice to practice.)

The Optomap system requires no initial cash outlay. Practices pay a pre-paid monthly fee based on an agreed upon number of scans.
Dr. Parker adds, "But even more important, it's generating word-of-mouth referrals from patients who are impressed with our technology."
About six years ago, Michael S. Rothschild, O.D., founder of West Georgia Eye Care in West Carrollton, Ga., knew he wanted the Optomap system because he felt it would be beneficial for his patients. He estimated his breakeven point and never looked back. "I didn't want to profit a lot from it. I just wanted to break even," he says.
In fact, all the practitioners we interviewed — although concerned about the bottom line — overwhelmingly emphasized the clinical benefits of ultra-widefield retinal imaging.
"Optomap screenings alone provide a nice ROI, but frankly any retinal camera can provide a nice ROI for screenings," notes Dr. Castleberry. "What surprised me are the additional exams and special testing procedures generated because I'm detecting more conditions with the Optomap than with my retinal camera."
Dr. Castleberry adds that Optomap Plus testing is typically covered by medical plans.
| Optomap-Enhanced Comanagement |
|---|
| "A long-time patient, who now resides in the Bahamas still comes to us for her annual eye care," recounts Wayne J. Goldschneider, O.D. "At her most recent exam, Optomap revealed a small, peripheral, operculated retinal hole in her right eye, with a cuff of fluid surrounding it. This was not present on previous Optomap scans, which have been done yearly for the last 5 years. I reviewed the Optomap scans with her and explained the serious nature of this finding. Being able to show the patient the hole was invaluable for educating her. "I felt it prudent that the patient see a retina specialist ASAP, but she explained she was returning to the Bahamas the next day. Fortunately, I was able to contact her optometrist in the Bahamas and e-mail the Optomap images to her. She then arranged a consult with a visiting retina specialist from Bascom Palmer Eye Institute in Miami." A compliant patient, regular screenings and technology that facilitates remote consults produced a positive outcome. |
Quick start-up guide
Bringing in a new screening/diagnostic instrument often requires adjustments to existing equipment, the office layout and patient flow, as well as technical training for staff and doctors. According to the practitioners we interviewed, installing the P200 or P200C was a simple process. In most practices, installation took one day, with another day or so dedicated to technical and professional training. "Most practices will find the learning curve short," Dr. Castleberry says. "In addition, Optos Academies are held frequently around the country for practices interested in learning advanced skills."
As for scheduling and patient flow, Dr. Parker says differentiating tech time and doctor time helped his practice adapt. "We had to understand that this test adds some time to the front end of an examination — the time with the technician — and saves time with the doctor. Net exam time is about the same."
According to Dr. Rothschild, visualizing and planning for the new system before it arrives will ease the transition. "Immediately start planning for the perfect scenario," he says. "Think about how it will change your patient flow and your pretesting. What will your technicians say? When will they say it? Practice what you'll say when you pull up the images on the monitor with the patient in the exam room. When the equipment is installed, you'll know what you're going to do, and you can make adjustments as you go."
Once you and your staff are educated, you'll need to turn your attention to how you'll present Optomap imaging to your patients.
Educating patients
How do these practitioners explain ultra-widefield screening to patients? "It's very simple," Dr. Rothschild says. "We just say, ‘This is our preferred way of evaluating the retina. It is a wide-angle digital image so that I can see your retina all at once. I can zoom in and move the image around and change the lighting so that I can study any imperfections that we find on the inside of your eye.’"
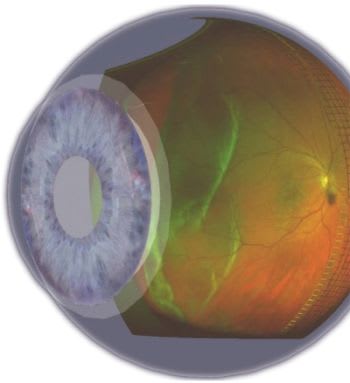
Several practitioners cited the educational benefit of the Optomap 3D Wrap feature. (See the image found at the top.) "I explain to patients that this revolutionary technology scans the retina edge to edge and is different from retinal photography, which shows only the central part of the retina and does not allow us to manipulate the image," Dr. Ossip says. "I can increase their understanding by using the 3D Wrap software tool, which shows the retina in a three-dimensional model eye. I explain that in a quarter of a second, we can obtain a scan that will show us any retinal problems that might indicate diabetes, hypertension, glaucoma, tumors or retinal detachments. Patients love being able to see their own eyes while learning about the retina."
A fundamental change
Providing ultra-widefield retinal imaging could be the differentiating factor that will take your practice to the next level.
"Optomap changed my practice to its core," Dr. Castleberry says. "It made advanced medical retinal services possible and profitable for my practice: Possible, because it makes me a better doctor, able to diagnose and treat a much wider range of serious vitreoretinal conditions; profitable, because my practice can now care for conditions that I referred to retinal specialists in the past. I know it can do the same for other O.D.s wanting to provide advanced medical retina services. It will benefit our patients by protecting their sight and enhancing their lives."
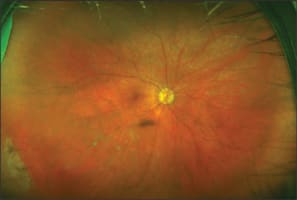
The Optomap reveals peripheral retinal conditions, including the snail-track degeneration shown here.
According to Dr. Ossip, the benefits of an examination using the Optomap technology are three-fold: "First, the user-friendly technology gives patients a real ‘wow’ experience. Second, doctors get great clinical information. Third, the practice develops a new initial revenue stream from the screening and a second revenue stream from medical optometry." OM