


CONTINUING EDUCATION
Dealing With Noncompliance and Ocular Surface Issues
Here's how persistent follow up turned a noncompliant patient into a compliant one and helped resolve ocular surface problems.
What good is effective glaucoma therapy if a patient refuses to use it initially and then, after using it to achieve positive results, decides not to use it anymore because of side effects? These are the issues I needed to address in the following case. Sometimes, we have to get a little creative in our approach to treatment and management of glaucoma to achieve positive outcomes.
Diabetes and Difficulty Driving
A 71-year-old Caucasian woman with a 5-year history of diet-controlled type 2 diabetes complained she had trouble seeing while driving at night. Her medical history included no allergies but her mother had been diagnosed with primary open-angle glaucoma.
Here are the findings from my initial physical exam:
■ Visual acuity: 20/60 OD, 20/50 OS
■ Manifest refraction: OD +1.50DS 20/25; OS +1.25-0.75×135 20/25
■ Pupils: PERRLA, absent relative afferent papillary defect (-RAPD)
■ Extraocular muscles: smooth and full
■ Color vision: within normal limits using AO plates
■ IOP: 25 mmHg OD, 26 mmHg OS
■ Gonioscopy, using the Ocular Sussman Four-mirror lens: D-40-R configuration OU (wide open to the ciliary body) with 2+ trabecular pigment 360 OU
■ Slit lamp examination: cornea, clear OU; anterior chamber, deep and quiet OU; 2+ nuclear cataracts OU
■ Dilated fundus evaluation: moderate cupping of both optic nerves but an intact neuroretinal rim, observed 360°. Rare "blot and dot" hemorrhages OU without clinically significant macular edema (CSME)
■ Threshold visual fields, using the Humphrey 30-2 program, were normal and reliable OU.
Prophylactic Treatment Refused
Even though the patient had normal visual fields and fairly normal optic nerve heads, I discussed with her the benefit of prophylactic treatment for ocular hypertension.1 I also discussed the risks of diabetic retinopathy and the possible risk of further progression without appropriate treatment.2 She refused to consider treatment for her ocular hypertension at that time.
In July 2001, she presented with no change in complaints, stable vision and slightly higher IOPs of 26 mmHg OD and 28 mmHg OS. The fundus exam showed nonproliferative diabetic retinopathy (NPDR) without CSME OU. She had moderate nerve head cupping and peripapillary atrophy OU.
The Ocular Hypertension Treatment Study (OHTS) suggests that elevated IOP is a significant risk factor in the development of open-angle glaucoma. IOPs above 21 mmHg and 22 mmHg generally prompt us to recheck IOPs at follow-up.
In this case, I was concerned that her optic nerve showed possible change over time, which was more obvious OS. This seemed to be supported by a visual field that showed a superior nasal depression and a superior nasal step in the left eye. With these factors in mind, I strongly recommended this patient start using glaucoma medication. But again, she refused despite significant patient education.
Progression Continuing
The patient returned in January 2002, with IOPs of 28 mmHg OD and 38 mmHg OS. I saw no changes in her optic nerve heads or visual fields. I explained to the patient that she probably would begin losing vision and potentially go blind if she continued to refuse treatment. She agreed to a monocular trial of latanoprost (Xalatan, Pfizer Inc.), qhs, for 3 weeks.
The medication reduced her IOP in her left eye from 38 mmHg to 19 mmHg, but the pressure in her right eye climbed 4 points to 32 mmHg. I convinced her to use the drops in both eyes, which eventually reduced her IOPs to 18 mmHg OD and 20 mmHg OS. These pressures were still above my target of the mid-teens or lower, so I added brinzolamide (Azopt, Alcon Laboratories Inc.).3 Some doctors might have added a beta-blocker, but I prefer adding a carbonic anhydrase inhibitor or, as a second choice, brimonidine tartrate 0.15% (Alphagan P, Allergen Inc.) to a prostaglandin.
Positive Response
In September 2002, the patient reported good compliance with her medications. Her IOPs were 14 mmHg OD and 13 mmHg OS. The OHTS findings now had revealed that reduced CCT was a powerful predictor for the development of primary open-angle glaucoma.4
Her CCT findings were 503 microns OD and 501 microns OS — very thin corneas in both eyes that classified her as a high-risk patient.
Her visual fields were normal and reliable OD but showed a superior nasal depression OS, revealing glaucomatous loss, despite good pressures.
The significance of CCT has been evaluated only in patients with elevated IOPs. In the OHTS, patients were evaluated with IOPs of 24 mmHg to 32 mmHg. For example, a CCT of 535 microns wouldn't be considered thin if a patient had suspicious cups and IOPs of 17 mmHg. But a CCT reading of 535 microns in an ocular hypertensive patient with much higher IOPs would be considered thin and therefore alarming. In the OHTS, 570 microns was the mean for patients whose pressures were 24 mmHg and above, and the average range was 555 microns to 588 microns. Any reading higher than 588 microns is considered thick. Any reading below 555 microns is considered thin. The hazard ratio doubles with every reduction of 40 microns. At a minimum, then, a patient's pressure has to be 24 mmHg or higher for you to avoid extrapolating too much from the OHTS.
Poor Compliance
The patient returned in January 2003 and reported spotty compliance, with complaints of a burning sensation upon instillation of the latanoprost, but she used the drop as suggested within the 3 weeks before my evaluation. Her physical exam revealed stable NPDR without CSME. Her IOPs were 10 mmHg OD and 9 mmHg OS.
The patient's visual fields were normal and reliable OD and revealed a dense superior hemifield depression OS, especially nasally. Her fundus exam showed moderate cupping of both optic nerves, with marked thinning of the inferior neuroretinal rim OS (Figure 1). Peripapillary atrophy was present OU. It was an optic nerve that appeared to be showing progressive glaucomatous damage.
I continued her existing treatment regimen due to her excellent IOPs and showed her the additional damage that occurred to her visual fields during her period of noncompliance. Over the next 2 years of follow up, the patient's IOPs remained stable at around 10 mmHg, and there was no change in the appearance of her optic nerve heads.
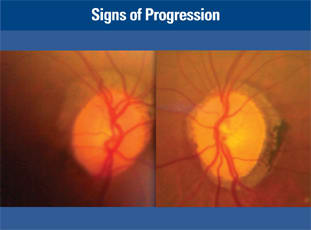
Figure 1. These fundus images show moderate cupping of both optic nerves, with marked thinning of the inferior neuroretinal rim OS.
Irritation Affecting Compliance
During a follow-up visit in August 2008, the patient reported good compliance but complained the burning associated with the latanoprost was getting worse. A slit lamp examination showed immediate tear film breakup time and superficial punctate keratitis. Her IOPs were 11 mmHg OD and 12 mmHg OS.
At this point, even though her treatment regimen was controlling her IOP, I obviously needed to respond to the increased stinging and ocular surface disease associated with the drops.5,6 I discontinued the latanoprost and prescribed travoprost with sofZia (Travatan Z, Alcon Laboratories Inc.). I also recommended she begin using the lubricant eye drop Systane (Alcon Laboratories Inc.) as needed.
Assessment and Prognosis
Currently, significant glaucomatous damage is evident in both the visual fields and optic nerve evaluation OS. However, the patient's IOP is consistently at target, and she's tolerating the travoprost. My plan is to maintain tight IOP control and carefully monitor her. I've emphasized to her that SLT laser surgery or surgical trabeculectomy are reasonable alternatives to medical treatment. She doesn't want to pursue surgery at this time.
This is a patient who could progress rapidly, despite aggressive IOP control. In cases like this, I perform visual fields every 6 months. Her pattern standard deviation (PSD) has remained stable after the rapid initial loss OS. I use PSD to determine if the patient has experienced focal loss, and I use the mean deviation to reflect the generalized depression.
Presently, the patient is comfortable and consistently compliant. As long as she stays compliant and maintains tight IOP control, we'll have the best chance of preventing future vision loss. OM
| References |
|---|
|