


binocular vision
Identify Binocular Vision Disorders
Millions of children and adults suffer unnecessarily from binocular vision disorders because they're underdiagnosed. Rectify this by following these four steps.
DOMINICK M. MAINO, O.D., M.ED., F.A.A.O., F.C.O.V.D.-A., Harwood Heights, Ill.
In comparison to glaucoma, cataract, age-related macular degeneration, diabetic retinopathy and dry eye syndrome; binocular vision (BV) disorders are even more frequently encountered than these diseases and have significant negative effects on one's quality of life. In fact, one study revealed that the prevalence of accommodative and BV (strabismic and non-strabismic) disorders is 9.7 times greater than the prevalence of ocular disease in children ages six months to five years old, and it's 8.5 times greater than the prevalence of ocular disease in children ages six to 18 years old.1 In addition, a study of 1,679 patients between the ages of 18 and 38 showed that 56.2% presented with symptoms associated with BV dysfunction.2 Although these are alarming statistics, a disconnect exists between the high prevalence of BV disorders in the general population and the BV patients reported being evaluated by primary care optometric practices.
To improve the lives of these often overlooked patients, while augmenting the financial health of your practice, follow these four steps.
1 Ask BV-related questions
Make sure your patient history form includes appropriate questions so you don't miss any possible BV disorders. To the best of my knowledge, no organization has developed a standard form primary care optometrists should use to assess the presence of BV disorders. Instead, most O.D.s adapt their forms according to those currently used by BV specialists to meet their practices' individual needs.
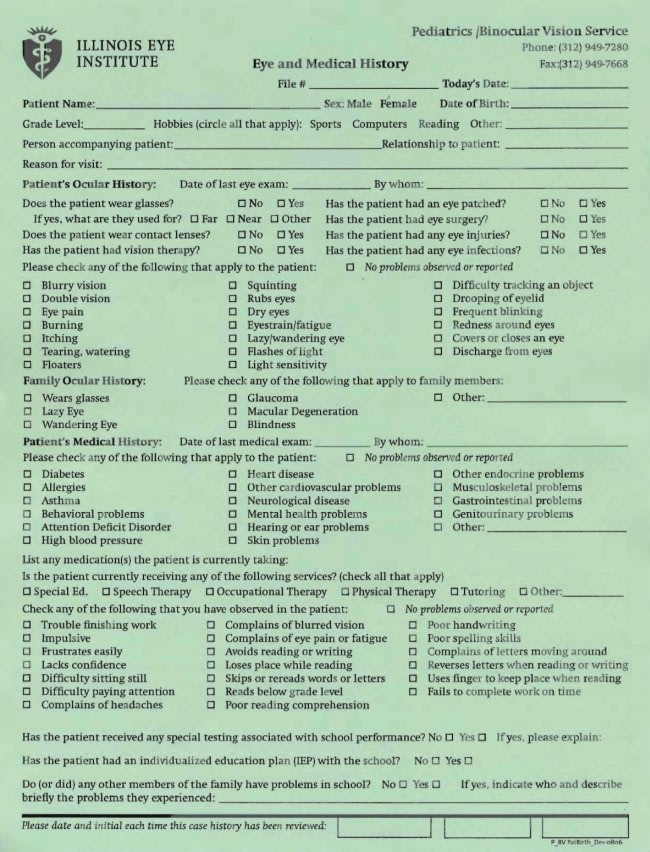
For instance, in my practice I provide several forms modified from the ones we use at the Illinois Eye Institute. These include the Illinois Eye Institute Eye and Medical History form for children, the Convergence Insufficiency Symptom Survey (http://www.minnesotavisiontherapy.com/UserFiles/File/Toni%20-%20Convergence%20Insufficiency%20Symptom%20Survey.pdf) and the College of Optometrists in Vision Development (COVD) Quality of Life Survey. I may also give my adult patients the COVD Quality of Life Survey along with an adult case history form that covers BV disorder symptoms.
The Illinois Eye Institute Eye and Medical History form for children inquires about double vision, squinting and eye tracking anomalies, among other BV-related symptoms. (See below.) The Convergence Insufficiency Symptom Survey is comprised of questions regarding the occurrence of specific symptoms related to reading and close work, such as tired eyes; while the COVD Quality of Life Survey requires the patient to rate the occurrence of various BV symptoms, such as headaches and dizziness.
2 Review the answers with the patient
Just because the patient fills out a form, doesn't mean he's done so correctly. In addition, all too often I find one or more blanks on the form(s) because the patient missed the question — a possible symptom of a BV disorder — didn't understand it, doesn't see how it's related to vision (general development questions, for instance) or wants to test me to determine whether I'm a thorough practitioner.
As a result, you should always review the answers to your BV form(s) with the patient and/or his parent or caregiver and, of course, ask the appropriate follow-up questions to ensure the forms are complete and correct.
For instance, if a patient complains of diplopia, ask him about its frequency, time of onset, whether he notes it at distance or near, whether it occurs during a particular time of day, during the performance of a particular task or tasks and whether it�s consistent or intermittent.
3 Perform appropriate testing
If the patient's complete and correct patient history data reveal that he may have a BV disorder, explain to him that you're going to conduct a comprehensive examination that includes appropriate tests so you can decide whether he needs additional testing. Be sure to mention to the patient, however, that the typical comprehensive examinations don't always yield enough information for you to determine the presence of a specific BV disorder or for that matter the most appropriate diagnosis to decide on the best course of action.
For the patients I see, I usually conduct a comprehensive examination that includes enough tests so that I can determine whether additional testing is required, while meeting all the requirements of various health insurance companies. I then re-appoint them for a visual efficiency evaluation if needed. I explain to my patients that some or all of the specialized testing may require that they pay out of pocket. In other words, I tell them not to necessarily expect insurance to pick up the costs.
So, what comprises this "visual efficiency evaluation?" The answer is a more in-depth assessment of oculomotor dysfunction, sensory and motor fusion, vergences and accommodation.
The saccadic function assessment often includes the Developmental Eye Movement (DEM) test (Bernell), while the cover-uncover test assesses motor fusion. These tests determine problems with accuracy of reading eye movements, as well as the presence of strabismus. (As a brief aside, you can often diagnose poor pursuit and saccadic skills subjectively using a +1 to +4 scale with +1 indicating very poor performance and +4 the very best [the DEM test provides a more objective evaluation]).
The sensory fusion assessment is often comprised of four tests: The Worth 4 Dot, Random Dot, Wirt Dot and Stereo Fly tests. These tests help to determine the presence of suppression, which often accompanies a BV disorder.
The motor fusion/vergence assessment is comprised of the near point of convergence (NPC) test, as well tests that determine whether a large heterophoria and reduced vergences at far and near are present. You may conduct these tests using Risley prisms (Veatch Ophthalmic Instruments) in the phoropter or by using the handheld prism bar out of the phoropter. The results of these tests help you diagnose the major vergence dysfunctions associated with convergence and divergence.
Finally, the assessment of accommodation consists of amplitudes, negative relative accommodation, positive relative accommodation, accommodative facility, determination of the Accommodative Convergence/Accommodation (AC/A) ratio and an assessment of the lag of accommodation. The amplitudes of accommodation tests reveal how much accommodation is present (e.g. accommodative insufficiency or excess). You can assess the amplitude of accommodation using several different methods including a minus lens, push up and pull away techniques, accommodative facility and the +/-2.00 flipper test. The positive relative and negative relative accommodative tests show how accommodation works under binocular conditions. Accommodative facility tests determine how easily focusing can change from distance to near and back again. You can assess positive relative and negative relative accommodation using +/-2.00 flippers and an appropriate near target. The AC/A ratio reveals how the accommodative stimulus and response are related (e.g: if a little accommodation results in a great deal of convergence). And, you can assess the lag of accommodation via the Monocular Estimation Method (MEM). (See "Specific BV Disorders," below.)
4 Determine the best course of action
Once additional testing yields a diagnosis, you must decide whether you feel comfortable treating the condition. Keep in mind that this comfort level should be in tune with your ability to provide the patient with the best treatment plan. (See "Managing Common BV Disorders," below.)
For instance, many primary-care optometrists may feel comfortable treating intermittent strabismus, but not constant unilateral, alternating or vertical strabismus; as this is something typically overseen by an optometrist who specializes in optometric vision therapy. As a result, the best course of action is often either to refer the patient to a colleague whom you know is an expert in treating the condition or to provide the patient with a list of names of specialists from which he can choose. You can find referral sources by contacting the American Optometric Association (www.aoa.org), College of Optometrists in Vision Development (www.covd.org), the American Academy of Optometry (www.aaopt.org), the Optometric Extension Program (www.oepf.org/) and your state optometric association.
I realize that several practitioners are reluctant to refer patients to another optometrist or, perhaps, ophthalmologist for fear of losing the patient to this individual. The ramifications of not doing so, however, can be devastating. In fact, during the crafting of this article, I've been a legal consultant in a case in which a colleague may have failed to treat or refer a child who has functional amblyopia appropriately. Do you really want to be in this situation? If not, then you need to appropriately diagnose, treat or refer these patients.
Through my experience, I've found that practitioners who specialize in vision therapy return a majority of these patients to the referring doctor's care once the patient has completed the therapy, or these patients return on their own. The latter often occurs if you explain to the patient that this particular condition falls out of the realm of your expertise and that you want to make sure he gets the best possible treatment. The patient often appreciates your honesty and commitment to his wellbeing so much, that he's sure to return to you for the other excellent eyecare services you provide.
Remember: We must treat and refer appropriately for all functional vision disorders or endure the consequences associated with patient dissatisfaction and even legal action.
For information on how to incorporate the diagnosis and management of BV disorders into your practice, look for articles in Optometry & Vision Development (http://www.covd.org/Portals/0/19-20Practice%20Management%20Wright.pdf) by authors such as Mark Wright, O.D. (www.covd.org/Portals/0/EvaluatingYourself.pdf), Jason Clopton, O.D., F.C.O.V.D. (www.covd.org/Portals/0/PracticeMgmt_ChangingParadigms.pdf) and Peds/VT Practice Management GuruThomas Lecoq (www.covd.org/Portals/0/OVD38_4_Practice_Management.pdf). Also, read the practice management chapters in BV textbooks by Scheiman and Wick, such as "Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders" (Lippincott Williams & Wilkins, 2008), and attend the yearly COVD programs.
Meeting the needs of patients who have BV disorders won't only enable you to better the lives of these often-ignored patients, but also grow your practice. This is because these patients tend to be so appreciative of and impressed by your diagnostic abilities, that they'll refer others whom they believe may have BV disorders as well. OM
| Managing Common BV Disorders |
|---|
| • Amblyopia. The best initial treatment for all types of amblyopia is a pair of spectacles, as glasses alone can significantly improve visual acuity. If after wearing glasses for a couple of months, the patient's improvement in vision isn't what you'd like, start a patching regimen consisting of two hours of daily patching that includes one hour of near visual activities. If the patient is noncompliant with patching, have him or his caregiver instill atropine ophthalmic drops in the better-seeing eye over a weekend (one drop on Saturday, another on Sunday). The result of doing so closely approximates that of patching. The one hour of near activities suggested above as a part of the treatment plan should include monocular (by patching or blurring/penalization), oculomotor handeye (i.e., filling in O's in a newspaper) and accommodation activities (i.e., Hart Chart Accommodative Rock Chart [www.nova.edu/hpd/otm/mba/vt/VTACC03.HTM]). Also, you may want to prescribe one of the many optometric vision therapy computer programs available for amblyopia. These include those from Home Therapy Solutions, Vision Builder and Computer Aided Vision Therapy. If after a reasonable time period — typically three months — your treatment outcomes have reached a plateau or you're unsure of the next step, refer your patient for a more aggressive in-office optometric vision therapy program. As a brief aside, be aware that the treatment of amblyopia isn't just appropriate for children but also for adults. In fact, current research in neuro- and cortical plasticity strongly suggests that an active therapy program (vision scientists refer to this as perceptual learning) can show significant improvement in the visual acuity of the adult patient. At the recent COVD meeting, Dennis Levi, O.D., Ph.D, dean of the school of optometry at the University of California, Berkeley, and respected vision scientist, noted that perceptual learning (vision therapy) can be both effective and efficient if intervention is intensive, active and challenging. His research showed that 50 hours of perceptual learning — which is equivalent to 25 days of two hours of patching with one hour of near vision therapy activities — boosts brain processing efficiency, decreases cortical image distortion and is appropriate for both the child and adult who has amblyopia. • CI. The recent Convergence Insufficiency Treatment Trial (CITT) revealed that the best and most efficacious treatment for CI is office-based vision therapy/orthoptics along with home-based therapy (i.e., Pencil Push-up therapy).3 Specifically, the results revealed that 12 weeks post-treatment, almost 75% of children ages nine through 18 who were given both forms of therapy achieved normal vision or had significantly less CI symptoms. Meanwhile, only 43% of those patients who completed the home-based therapy alone, 33% who used the home-based therapy in addition to computer vision therapy/orthoptics and 35% who underwent placebo office-based therapy had similar outcomes. You should also keep in mind that most children ages 9 to 17 years who were asymptomatic after the 12-week treatment program of office-based vergence/ accommodative therapy for CI maintained their improvements in symptoms and signs for at least one year post treatment.4 (For an audio/visual presentation regarding this ground-breaking research visit http://progressive.uvault.com/pd1005/COV081/07/player.htm). • Intermittent strabismus. The most appropriate treatment for these disorders frequently includes prescribing spectacles, prism, and, initially, out-of-office therapy. Eventually, however, in-office vision therapy may be required. If after three months or so your patient doesn't seem to be improving, it's time to refer to an optometric vision therapy specialist. Many primary care O.D.s may believe that referring patients who have a constant unilateral, alternating or vertical strabismus for surgery is the best course of action rather than referring these patients for vision therapy. Studies suggest, however, that surgical outcomes may not be as good as most of us might believe. The case of "Stereo Sue" (Sue Barry, Ph.D.) is a good example.5-7 She was born with strabismus and underwent multiple surgeries to correct it. While the surgeries almost fixed the appearance of her strabismic eyes, they didn't correct the visual problem. Ultimately, vision therapy provided her with stereopsis and 3D vision. Further, one surgical study showed that 13 years postoperatively no outcome was "very good," four were "good," 12 were "satisfactory," and two were "poor."8 Very good was defined as orthophoria or orthotropia with exophoria or esophoria of less than 5PD. Good was defined as exophoria or esophoria less than 10PD or orthotropia of 5° (microstrabismus). Satisfactory was defined as exophoria or esophoria greater than 10PD or exophoria or esotropia greater than 10PD but less than the preoperative angle. Finally, poor was defined as the same as the patient's preoperative condition or worse. |
| Specific BV Disorders |
|---|
| • Convergence insufficiency (CI). A patient who has this BV disorder may have one or more of the following: a receded NPC, an exophoria at near, reduced positive fusional vergences and/or a deficit in NRA. Although seeing all the above in any single patient is unusual, you�ll almost always note the presence of a poor NPC and high exophoria at near. • Convergence excess (CE). A patient who has a near deviation of at least 3 prism diopters (PD) more esophoria than at distance and which may be associated with a high AC/A has CE. • Divergence insufficiency (DI). This rare BV disorder, which may have a non-functional pathological/organic etiology (rule out divergence paralysis and unilateral or bilateral sixth cranial nerve palsies), occurs when esophoria is greater at distance when compared with near. Many of these patients have low fusional divergence amplitudes at distance and reduced AC/A ratios. • Divergence excess. This occurs when the patient's exophoria is greater at distance than at near. Many of these patients have low fusional divergence amplitudes at distance and reduced AC/A ratios. Also, they're often asymptomatic but may report intermittent diplopia when going from a dark to a lighted environment (i.e., from a darkened movie theater into the sunlight). • Basic exophoria and basic esophoria. These conditions show an equal amount of deviation at distance and near. You can note these BV disorders when the patient's heterophorias are normal but significantly reduced vergence ranges are present. These patients demonstrate a very limited zone of single clear binocular vision. • Accommodative insufficiency. When the amplitude of accommodation is low or you note a high MEM finding for the non-presbyopic patient's age, he has this BV disorder. • Ill-sustained accommodation. A patient with this disorder has normal accommodative amplitudes but shows rapid fatigue when you place repetitive demands upon the focusing system. • Accommodative infacility. This disorder occurs when the focusing system is slow in shifting from distance to near and back again or when a substantial delay occurs between the stimulus to accommodation and the response. • Accommodative excess or spasm of accommodation. This disorder results from overstimulation of the parasympathetic nervous system, and it's frequently related to overall fatigue. The condition is also sometimes known as the spasm of the near reflex (disproportionate accommodation, overconvergence and miotic pupils). Accommodative excess can result from cholinergic drug use, trauma, a brain tumor or myasthenia gravis. • Strabismus. The most often diagnosed forms of strabismus include exotropia and esotropia. You may notice vertical anomalies, a hyper or hypodeviation, but you usually don�t encounter these conditions as frequently as horizontal deviations. Optometrists tend to encounter traumatic and/or disease-caused strabismus less often than functionally induced misalignment of the eyes. However, this may now change with the growing interest by optometrists in working with acquired brain injury patients. • Form deprivation amblyopia. This type of amblyopia occurs when an obstruction along the line of sight stops the formation of a well-focused, high-contrast image on the retina. Congenital cataract is the most frequent etiology of this type of amblyopia. Strictly speaking, this isn't a true form of amblyopia since it isn't of a functional nature but rather has a pathological and/or organic etiology. • Refractive amblyopias. These are comprised of isoametropic amblyopia, which a roughly equal, high magnitude uncorrected bilateral refractive error causes, and anisometropic amblyopia, which has an etiology of demonstrating a significant uncorrected refractive error difference between the two eyes. • Strabismic amblyopia. This is associated with an early onset constant (early childhood) strabismus. |

|
Dr. Maino a professor of pediatrics/ binocular vision at the Illinois Eye Institute/Illinois College of Optometry, is the editor of Optometry & Vision Development and authors the blog MainosMemos, in which he reviews the latest children's vision research. Also, he's in private practice in Harwood Heights, Ill. E-mail him at dmaino@ico.edu. |
- Scheiman M, Gallaway M, Coulter R, et al. Prevalence of vision and ocular disease conditions in a clinical pediatric population. J Am Optom Assoc. 1996 Apr;67(4):193-202.
- Montés-Micó R. Prevalence of General Dysfunctions in Binocular Vision Annals of Ophthalmology, 2001 Sept;33(3):205-208.
- Clinical Studies Database. Supported by the National Eye Institute. Convergence Insufficiency Treatment Trial. www.nei.nih.gov/neitraisl/viewStudyWeb.aspx?id=107. (Accessed 11/09).
- Convergence Insufficiency Treatment Trial Study Group. Long-Term Effectiveness of Treatments for Symptomatic Convergence Insufficiency in Children. Optom Vis Sci 2009 Sept; 86(9):1096-1103.
- Sacks o. A Neurologist's Notebook, "Stereo Sue," The New Yorker, June 19, 2006, 64-73.
- Barry SR. Essay: Stereo views. Optom Vis Dev 2006: Feb; 37(2):51-4.
- Press L. The story behind 'Stereo Sue' and a world-famous neurologist's discovery of vision therapy. Optom Vis Dev 2006 Feb; (37) 2:55-57.
- Kordic H, Sturm V. Landau K. Long-term follow-up after surgery for exodeviation. Klin Monatsbl Augenheilkd. 2009 Apr;226(4):315-20.