


CONTINUING EDUCATION
Administering Clinical Therapy for Ocular Allergy Patients
Here's how you can provide relief to millions of patients with a new class of medications.

By Arthur Epstein, OD, FAAO
In the past few years, we've made great strides in our understanding of allergy. We've learned that allergy is a very complex ocular disorder — much more complex than we thought in the past. We know that a combination of heredity and common environmental factors, such as pet dander, trees, grasses, dust mites and pollen cause allergies.
Clinically, we know that allergy manifests as a specific form of inflammatory ocular surface disease, which is key to understanding the etiology and treating the disorder. The mast cell is the primary cell involved in the allergic response, but not the only one. And while histamine that binds to H1 receptors is the chief initiator of the allergic response, again, it's not the only one.
This broader understanding has led to new therapeutic approaches, which in turn empower us to better treat our patients. In this article, you'll learn about the opportunities you have as a clinician to treat ocular allergy. You'll learn about the key signs and symptoms of the most common types of allergy and the latest strategies to treat them.
Opportunity Knocks
Ocular allergy has been a fascination of mine for well over a decade, because it's had the power to move the field of optometry from a refractive profession to a therapeutic profession. Allergy presents a huge opportunity for us to improve our patients' lives and enhance our practices. It's estimated that at least one quarter of the population suffers from allergies.1 In my experience, many, if not the majority, of these patients have ocular components to their allergies. However, few of these ocular allergy sufferers who could benefit from topical medications actually receive them.
When patients use modern drops with antihistaminic properties, they get relief within a few minutes. This fast relief strengthens the patient-physician relationship that's built in a therapeutic practice, because patients tie the prescription's success directly to our clinical acumen.
In short, allergy is significant because it's everywhere. We live with pets we love, sleep in beds filled with dust mites and enjoy the outdoors filled with pollens. The eyes are particularly susceptible to allergens because they're directly exposed to the environment, without the filters of the respiratory system. The highly vascularized conjunctiva presents a rather large surface area for allergens and contains large numbers of mast cells.
Allergy Types, Signs and Symptoms
Patients may present with any combination of the five types of ocular allergy: seasonal allergic conjunctivitis (SAC), perennial allergic conjunctivitis (PAC), giant papillary conjunctivitis (GPC), vernal keratoconjunctivitis and atopic keratoconjunctivitis. SAC and PAC affect about 95% of optometric patients with ocular allergy, making these the essential focus for optometrists who want to expand the therapeutic side of their practices.2
The signs and symptoms of SAC are well known:
• Itching. This number-one complaint is the key to distinguishing allergy from other types of ocular surface disease, and it's most significant for patients who experience the discomfort.
• Redness. Appearances count. The ocular redness associated with allergy often is very disturbing to patients.
• Chemosis, lid swelling and tearing. Puffy, watery eyes may accompany the itching and redness.
SAC often is an outdoor allergy, yet the allergens often find their way indoors through air vents in buildings or on our clothing and hair. On the other hand, PAC is a year-round condition triggered by animal dander and dust mite feces. The signs and symptoms of PAC are generally the same as SAC, although they're typically milder.
Mast Cells, the Allergic Cascade
Mast cells are the key cells involved in the allergic response. Historically, they've stood as fortresses waiting for an opportunity to wage war against life-threatening parasitic infestation. Today's allergic responses to common allergens in our environment are thought to be related to epidemics of parasitic infestation that occurred thousands of years ago.3 Our allergy patients are the survivors of these epidemics.
Degranulation of mast cells triggers the allergic cascade. First, an antigen, such as pollen or dander, comes into the field. The mast cell, which has been presensitized by prior contact with an allergen, becomes coated with IgE-receptors that bind to the antigen, causing the mast cell to degranulate. As degranulation occurs, mast cells release a number of mediators, such as histamine, the most common allergic mediator. Keep in mind that other mediators, such as tryptase, heparin and prostaglandins, are either released or synthesized by the mast cell, which believes it's fighting a life and death battle.
There are four different types of histamine receptors in the body, but only one (H1) plays a role in the eye. Histamine binds to H1 receptors on the nerves, causing itching, and it binds to blood vessels, causing redness and chemosis (Figure 1).
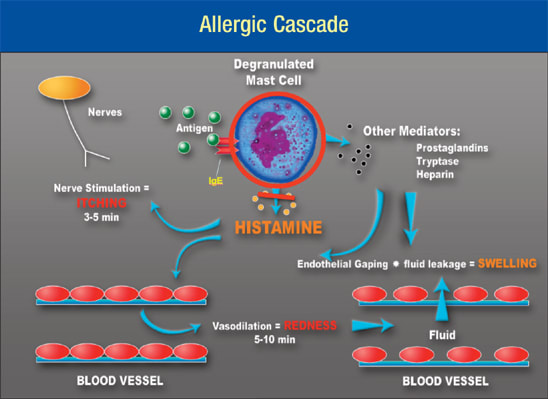
Figure 1. The mast cell is the central cell in the allergic response. The antigen (pollen, animal dander, etc.) cross-links to the IgE receptor and causes the mast cell to degranulate. Degranulation causes the release of histamines and other proinflammatory mediators, such as prostaglandins, tryptase and heparin. Histamine is the primary mediator that binds to the H1 receptors on the nerves (causing itching) and blood vessels (causing redness and chemosis).
Therapy for Ocular Allergies
Several topical agents with antihistaminic properties are available for the primary treatment of allergic conjunctivitis:
• Antihistamines such as emedastine (Emadine, Alcon Laboratories Inc.) are still a common allergy treatment in some countries, but they only block the action of histamine. They have no effect on the actions of other mediators that cause ocular symptoms. Patients get significant, but not complete relief.
• Mast cell stabilizers perform as their name implies. They stabilize mast cells to prevent them from releasing histamines and other mediators, thereby shutting down the allergic cascade at the source. They include medications, such as cromolyn (Crolom, Bausch & Lomb), lodoxamide (Alomide, Alcon Laboratories Inc.) and nedocromil (Alocril, Allergan Inc.). I should note that all of the available mast cell stabilizers were designed for respiratory allergy. Mast cell populations differ between the surface and deeper tissues like the respiratory system and the gut. Since medications behave differently depending on the mast cell subtype, some experts believe that these traditional mast cell stabilizers are largely ineffective against SAC and PAC.
• Nonsteroidal anti-inflammatory drugs (NSAIDS), such as ketorolac (Acular, Allergan Inc.), primarily work to inhibit itching, although they've been superseded by equally safe and more effective combination topical allergy medications.
• Steroids such as loteprednol etabonate (Lotemax, Bausch & Lomb) are effective against allergic inflammation. However, with the exception of the more severe cases, it's better to use the newer combination agents, which are disease-specific and have much better safety profiles. You should use steroids Allergic Cascade with caution when treating chronic disorders.
• New combination antihistamines. In 1997, the introduction of olopatadine (Patanol, Alcon Laboratories Inc.) marked a paradigm shift in the way we treat and manage allergy. Combination agents, such as azelastine (Optivar, MedPointe Pharmaceuticals), ketotifen (Zaditor, Novartis Ophthalmics) and epinastine (Elestat, Allergan Inc.) have strong antihistaminic effects, as well as greater mast cell stabilization. We went from patients taking two medications four times a day to patients taking a single medication twice a day and now once a day. The decreased dosing changed the way patients responded, and altered the way we manage them.
Antihistamine Effects
We tend to think that topical ophthalmic antihistamines simply work on histamine receptors. This is true, but they have a number of other effects as well. The effects of greatest concern to us as eyecare providers are: histamine receptor antagonism, anti-inflammatory effects and biphasic mast cell membrane stabilization.4
1. Histamine receptor antagonism. When histamine binds to a receptor on nerve or vascular cells, it produces the signs and symptoms of allergy. Antihistamines are inert molecules, stereochemically identical to histamines. However, antihistamines have a much greater affinity to receptors than histamine does, so they displace the histamine and shut down the allergic response. In fact, at marketed concentrations, antihistamines have much greater affinity for H1 receptors than histamine does. That explains the ability of antihistamines to stop the allergic response.
2. Inflammation. In the past, we thought of the mast cell as the leading actor in allergy, but now we understand that receptors on ocular surface epithelial cells play an important modulatory role in the overall allergic response. A current strategy is to inhibit the allergic response with antihistamine drops. One study5 showed that some topical ocular drugs "may offer therapeutic advantages … by inhibiting proinflammatory cytokine secretion from human conjunctival epithelial cells." That is, some drugs may have significant inflammation-inhibiting effects beyond those of antihistamines alone.5
3. Biphasic membrane stabilization. First described by Mota and da Silva6 in 1960, H1 antihistamines inhibit the release of mast cell mediators independently of H1 receptor activity.
These researchers were trying to understand why antihistamines seemed to have a much greater clinical effect than one would predict based on the pharmacokinetics and pharmacodynamics of histamine-antagonists. They conducted a series of experiments and discovered that in addition to the histamine-antagonist effects, antihistamines also have other nonspecific influences on whole cell membranes.
The data showed that at low concentrations, antihistamines stabilize cell membranes, and at high concentrations, they destabilize cell membranes. This stabilization occurs through a process called intercolation. At low concentrations, antihistamines act as splints to stabilize cell membranes, and at higher concentrations they show detergent-like effects disrupting cell membranes.
Combination Drugs
Traditional antihistamines block almost all of the allergic response, but they don't stabilize the mast cell and inhibit degranulation in commercial concentrations. The goal of new combination drugs is to achieve some mast cell stabilization along with the other benefits of antihistamines. Some combination drugs achieve this goal more effectively than others.
Current therapeutic options include azelastine, ketotifen, epinastine and olopatadine. The majority of optometrists prescribe olopatadine. Most drugs don't maintain such a high market share for a decade, unless they're the only product on the market. But we have a number of drugs in this category. This suggests there's a difference between products. However, no one medication works for everyone, although at least one appears to be highly effective for most of our patients.
In one in vivo study, pretreatment with epinastine and olopata dine significantly reduced clinical scores and eosinophil numbers.7 However, when we examine the biphasic effects of the combination drugs, we see that all of them except for olopatadine follow the prototypical antihistamine pattern. That is, the drugs inhibit histamine release at low concentrations, but disturb the cell membranes at higher concentrations, triggering further histamine release. Olopatadine inhibits histamine release without disturbing cell membranes.8,9
Other differences exist as well. In a further comparison of epinastine and olopatadine, patients said their eyes felt more comfortable when they instilled olopatadine drops, both immediately and after 5 minutes.10 Instillation comfort is especially important in a drug that targets discomfort.
Optometrists have two choices for olopatadine: olopatadine 0.1% (Patanol) twice a day or olopatadine 0.2% (Pataday) once a day. For some patients, the convenience of a reduced dosing schedule may increase compliance, leading to better symptom control and satisfaction. 11,12
In one study,13 patients leaned favorably toward the higher-concentration once-a-day dose of olopatadine. Researchers administered olopatadine 0.2% to 330 patients who previously had used olopatadine 0.1%. About 78% said olopatadine 0.1% was satisfactory, but after 4 weeks of using olopatadine 0.2%, 88% of patients rated the new once-a-day drug superior to the lower concentration.
Key to Effective Therapy
How can you make your patients happier? How can you satisfy their needs? How can you improve the quality of their lives?
Every allergy patient wants rapid symptomatic relief. That's antihistaminic activity for relief within 3 minutes. They also want long-term relief. That's prophylaxis, or cell stabilization. Patients want topical administration, not systemic antihistamines that can cause sleepiness and ocular dryness. And finally, patients don't want to use a drug throughout the day.
New combination drugs are your best chance at meeting patients' needs. They have an enormous advantage over older antihistamines because they attack allergy from a broader perspective. They block allergy at the right point to shut down the entire cascade, including primary and secondary inflammation. This clearly differentiates them from the older antihistamines.
In my practice, greater comfort and reduced dosing frequency are positive factors. Patients believe the drug is working better if they need to use it less often, and they say this improves their quality of life — a major issue for allergy patients. When medications are easier to take, patients are more likely to comply and achieve better results.
That's why, going forward, I believe combination drugs will help meet the key goals of effective allergy therapy. It's important to understand that most patients have been underserved in this area, and effective treatment will keep them coming back. You must acknowledge that patients and doctors benefit from convenient therapeutic delivery. And most importantly, you must remember that it's about the patient, and the patient's needs and goals must drive all of your treatment decisions. OM
Arthur Epstein, OD, FAAO, is a founding partner of North Shore Contact Lens & Vision Consultants, Long Island, NY. He's past chair of the American Optometric Association's Contact Lens & Cornea Section and is a clinical adjunct assistant professor at Northeastern State University College of Optometry, Tahlequah, Okla.
| References |
|---|
|