


contact lenses
Perfect The Football Fit
Follow these astigmatic lens option tips to ensure successful outcomes.
DIANNE M. ANDERSON, O.D., F.A.A.O., Aurora, Ill.
Successfully fitting an astigmatic patient in a contact lens is like fitting puzzle pieces. It can be challenging and time consuming, but the end result is very rewarding. In an effort to make these lens fits more productive and less time-consuming, here are some tips on how to facilitate the fitting process with the currently available lens options.
Keep in mind that the type of astigmatism (i.e. regular or irregular) dictates your lens choice. As a result, the ability to evaluate corneal topography maps is an essential starting point. With-the-rule (WTR); against-the-rule (ATR) and oblique are all forms of regular astigmatism. (See figures 1a, b and c, below.) Irregular astigmatism results from keratoconus; pellucid marginal degeneration (PMD); Terrien's marginal degeneration; post-refractive surgery ectasia; post-penetrating keratoplasty; post-corneal trauma; and post-corneal transplant.
Differential diagnoses include corneal warpage, corneal compromise (due to tear film deficiency) or contact-lens-related conditions, such as corneal infiltrates and staining. In these cases, the patient's astigmatism will change as the cornea normalizes. Follow these patients with bi-weekly topography maps and refractions until you achieve a stable refraction and can begin the fitting process.
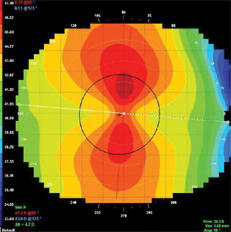
Figure 1a: With-the-rule astigmatism |
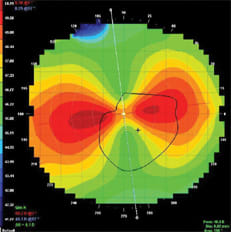
Figure 1b: Against-the-rule astigmatism |
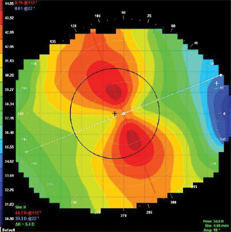
Figure 1c: Oblique astigmatism |
Patients who have regular astigmatism benefit from soft toric and GP lenses. Those who have irregular astigmatism achieve success in both GP and specialty lens designs.
Regardless of which lens you choose, educate the patient that finding the "right lens" is often a process due to the unique shape of his cornea. Then, assure him that you're going to use your knowledge in fitting to expedite the process. Finally, tell the patient what to expect at both the outset and as the fitting process unfolds. This not only keeps him motivated to achieve contact lens wear but also precludes him from seeking care elsewhere.
Soft toric lenses
A soft toric lens can rotate on the cornea. If rotation occurs, the patient experiences transient blur with each blink. To prevent this, measure the cornea's horizontal visible iris diameter (HVID). Doing so provides you with an idea of the corneal sagittal height — a measurement needed to determine the best lens base curve and diameter. (See figure 2 below). The average HVID is approximately 11.8mm.1 Determine the "Effective K" value of the cornea by adding 1.00D to the central corneal power (K) for every .2mm greater than 11.8mm and by subtracting 1.00D from the K for every .2mm less than 11.8mm.1 This concept is based on sagittal height rather than on K.
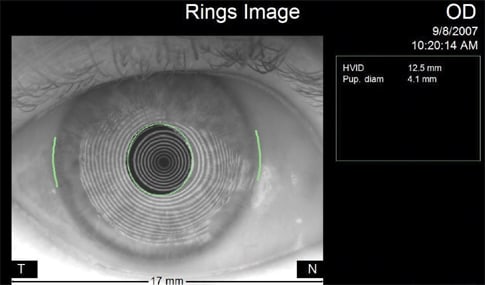
Figure 2: HVID of cornea measured via topography
For example, a 12.0mm cornea that has a 43.00D central K has an "Effective K" of 44.00D, and a 11.4mm cornea with a 43.00D central K has an "Effective K" of 41.00D. Therefore, a 12.0mm cornea with a 43.00D central K (apical radius) is better fit with a steeper soft toric lens than a 11.4mm cornea with a 43.00D central K. This concept is very important for a physiologically sound lens-to-cornea relationship and for the rotational stability of a soft toric lens.2
Once you've fit the selected lens, evaluate the lens power and axis, as spectacle prescriptions don't always translate to the contact lens, and lens rotation may be causing acuity and comfort issues. Use the LARS (left-add, right-subtract) method, which compensates for toric lens rotation by refining the axis. (Note: Be aware of the patient's refractive cylinder as compared with corneal cylinder. If corneal toricity is significantly less than refractive cylinder, a back surface soft toric lens may result in an unstable fit. Therefore, when managing these patients, consider a front surface toric GP lens design to improve fit and visual acuity.)
If the LARS method doesn't provide stable, clear vision, employ the SCOR (Sphero-Cylinder Over-Refraction) method. Patients who have high cylinder powers and require small axis refinements benefit from this method. Combine the over-refraction power and lens power using loose trial lenses, and neutralize those two lens powers together with a lensometer. Then, order a new lens in the resultant power.
If SCOR is unsuccessful, refit the patient in a custom soft toric or specialty lens design. Custom soft toric lenses are available in a much wider range of parameters than standard soft toric lenses.
GP lenses
A spherical GP lens may work well in cases of apical astigmatism, in which the cylinder is confined within the pupillary zone. This type of fit conforms well to the cornea by vaulting the steeper central area of cylinder and matching the flatter spherical periphery. If a spherical GP fit results in peripheral binding or 3 o'clock and 9 o'clock staining, however, refit with an aspheric GP lens. Doing so flattens the peripheral alignment. An aspheric GP lens is fit steeper than the flat K to maintain the proper sagittal depth while flattening the periphery.
In cases of limbal-to-limbal astigmatism, in which the corneal toricity extends to the limbus (see figure 1a, above), toric peripheral curves (PC) on a spherical lens help stabilize the fit by increasing the edge lift in the flat meridian and decreasing the edge lift in the steep meridian. The toric PC's help maintain the path of least resistance along the vertical meridian and points of bearing along the horizontal meridian.
If, however, corneal toricity exceeds 2.75D, fit the patient in a bitoric GP lens. Bitoric GP lenses provide the best fit and visual outcome in cases of great amounts of corneal cylinder.
Select a front surface toric lens only when the patient's cornea is spherical and the refractive cylinder is significant enough that the spherical equivalent produces inadequate acuity. Therefore, initially order a spherical GP, and evaluate the residual astigmatism upon dispensing. Keep in mind, however, that an over-refraction of this patient may result in residual astigmatism. On the contrary, the patient may experience good visual acuity with the spherical equivalent or "friendly flexure" of the GP material.
Don't fit a front surface toric GP lens on a patient who achieves enough visual acuity in a spherical lens, as front surface toric GP lenses are prism-ballasted and, as a result, can cause increased edge awareness on the lower lid.
Hybrid lenses
If corneal toricity is equal to or greater than the refractive cylinder, consider the SynergEyes hybrid lens (SynergEyes, Inc.). This lens consists of an 8.4mm, 100Dk RGP center with a 27% water skirt and an overall diameter of 14.5mm. The SynergEyes A (ametropia) and SynergEyes M (multifocal) lenses can correct up to 1.75D of regular astigmatism. Increasing the center thickness of these lenses with an "enhanced profile" can further correct the cylinder. And since the "A" and "M" lenses are spherical, rotational instability isn't an issue (see figure 3, below).
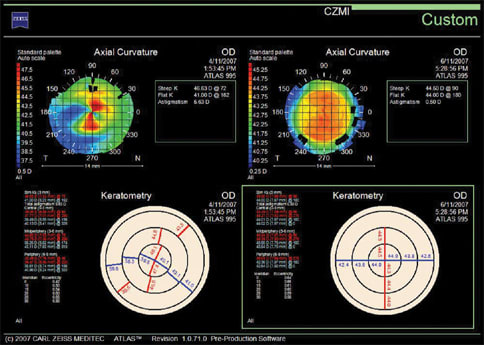
Figure 3: Custom display illustrates how irregular astigmatism (image = upper left/keratometry graph = lower left) can be masked by an enhanced profile SynergEyes A lens (image = upper right/keratometry = lower right).
Also, SynergEyes lenses can mask great amounts of irregular astigmatism, as in cases of keratoconus and PMD. The central portion of this lens is fit steep, which vaults these irregularities, and the soft skirt keeps the lens centered.
The SynergEyes KC (keratoconus) lens has an aspheric back surface. Further, this lens is available in an enhanced profile (increased center thickness), so you can control residual astigmatism in the keratoconic patient.
We work on puzzles for the reward of feeling great accomplishment when we fit that final piece. To acquire that reward efficiently, we scrutinize the puzzle box photo and use methods, such as picking out the edge pieces and separating pieces into color.
By using the astigmatic lens fitting tips outlined, you'll not only quickly obtain the reward of self-accomplishment, but patient loyalty and referrals, which will grow your practice. OM
1. Caroline PJ, Andre MP. Contact Lens Case Reports: Using HVID and Central K Readings to Design a Custom Lens: Contact Lens Spectrum. www.con tactlensspectrum.com/article.aspx?article=&loc=archive\2002\june\0502056.htm. (Accessed Jan. 2, 2009)
2. Bergenske, P. Prescribing Soft Toric Contact Lenses: Prescribing soft torics is easier than you might think and is a skill that benefits many of your astigmatic patients. Contact Lens Spectrum. www.contactlensspectrum.com/article.aspx?article=&loc=archive\2005\February\0205033.htm (Accessed Jan. 2, 2009).

|
Dr. Anderson practices in surburban Chicago, specializing in orthokeratology, keratoconus, post-surgical lens fits and anterior segment disease. E-mail her at dianne.anderson@comcast.net. |