


coding
E/M vs. Eye Codes: Which Should You Use?
This first in a three part series on coding explains E/M requirements.
RIVA LEE ASBELL, Fort Lauderdale, Fla.
One of the most difficult choices for most ophthalmic practitioners is deciding which set of codes to use — the Evaluation and Management (E/M) codes or the Ophthalmology (Eye) Codes. The ophthalmic practices are the only specialties with the privilege of choosing from two sets of codes for coding office encounters. This series, which will run in three parts, will help you, the optometrist make the correct choice.
Here, in Part I, I present an overview of the E/M requirements. Part II will provide an overview of the Eye Codes, and Part III will offer an algorithm guide for making "The Choice."
Background of E/M and eye codes
Many practitioners prefer using the Eye Codes, believing they are easier to use and more audit-proof. This is not necessarily so. If you use only eye codes, not only are you punishing yourself financially, but you also may be found to be upcoding or down-coding under audit. For example, the intermediate eye code for established patients (CPT code 92012) isn't always suitable for coding frequent follow-up visits, such as a follow-up examination for a corneal abrasion. (The correct code for healing a corneal abrasion is often E/M code 99212).
The objective, and what Centers for Medicare and Medicaid Services (CMS) wants, is for you to code correctly — to neither upcode nor downcode.
With the increase in CERT (Comprehensive Error Rate Testing) audits and the advent of the RAC (Recover Audit Contractor) audits, proper selection and correct and complete chart documentation takes precedence over everything else.
E/M codes
CMS first established the new E/M codes in 1994-1995 with the examination requirements for single organ systems (such as eyes) presented in 1997. The original document, "Documentation Guidelines for Evaluation and Management Services" jointly issued by the American Medical Association (AMA) and the Health Care Financing Administration (HCFA) (now CMS) may be found at: www.cms.hhs.gov/medlearn/emdoc.asp.
It was, and remains, difficult to learn the first time, but it has its advantages in that it's very black and white compared with the eye codes, which contain gray areas. It's very beneficial to master them. If used properly with a forced entry form for chart documentation, E/M codes become easy to master. (More on the chart examination form later.)
E/M codes are defined by seven components. The first three are used in conjunction with each other to determine the code for outpatient office visits/consultations. They elevate in levels of severity from one to five, with five being the highest, or most severe. These components are: History, Examination and Medical Decision Making. Some important points for each follow.
KEY COMPONENT 1: History
The First Key Component, the History, contains four component parts. They are:
► Chief Complaint
► History of the Present Illness (HPI)
► Review of Systems (ROS)
► Past History, Family History, and Social History (PFSH).
If you think of these components as a corporate organization chart with History — the First Key Component as the chairperson of the board and the following four components as vice presidents, you will understand it better.
• Chief Complaint. The chief complaint is the reason for the encounter, which may be in the patient's words or the history taker's documentation of the dialogue. This varies significantly from what most practitioners are taught — namely, that the chief complaint must be in the patient's own words.
Medicare doesn't cover services performed for annual checkups, routine visits, screenings, refractions or eyeglasses. If your chart note states that the patient's reason for coming in today is any of the following — "glasses aren't good," "routine checkup" "annual check" or "no real complaints" — then that automatically makes the service a non-covered one that the patient must pay for and for which the practice may not bill Medicare.
Take this test: If you self-audited last week's charts, would you pass or would you be refunding money to Medicare?
• HPI. The HPI is composed of eight elements that I commonly refer to as the brain-killers. They are: location, duration, timing, quality, context, severity, modifying factors, associated signs and symptoms.
The HPI is leveled into Brief and Extended, Brief having one to three elements described and Extensive having four or more elements described.
Why is this so important?
In order for an encounter to qualify as level 4 for the History portion, you must have an extended HPI — 4 or more elements must be qualitatively described. If you only describe three elements, the entire encounter drops to a level 2 and for a new patient, for example, you will have lost $83.12 on a national average.
You must address the eight elements and not repeat the same ones for credit. For example, with a complaint of blurry vision you can't count occasional tearing and itching as two elements. They both are examples of associated signs and symptoms.
Below is a bad example of a Chief Complaint (CC) followed by a good example.
CC: Patient complaining of red right eye with associated pain.
CC: Patient complaining of pain and redness in the right eye x one day. Sudden onset. Very severe. Also has nausea and abdominal pains.
• ROS and PFSH). The ROS and PFSH are basically inventories — you are taking an inventory of organ systems in the ROS and of the various pertinent occurrences in PFSH. It's pretty much like taking an inventory of your house.
The systems are: Constitutional — Eyes, Ears, Nose, Mouth, Throat; Cardiovascular — Respiratory; Gastrointestinal; Genitourinary; Musculoskeletal; Integumentary (skin and/or breast); Neurological; Psychiatric; Endocrine; Hematologic/Lymphatic; and Allergic/Immunologic.
In order to be in compliance with the proper chart documentation, you must note whether each system has been inventoried and whether the patient had any abnormalities. If you note an abnormality, you must describe it.
Chart documentation problems occur when the history taker fails to note normal or abnormal for each system and only notes the abnormalities.
One of the biggest problems I have encountered with coding is when the practice's history form uses disease entities, rather than organ systems. Thyroid and diabetes both belong in Endocrine, and cancer is not an organ system at all.
For the PFSH, you must ask one question for each category in order for that category to be considered inventoried.
Both the ROS and PFSH are leveled. To bill the higher level codes (Levels 4 and 5), you must inventory 10 or more organ systems for the ROS, and ask one question in each of the three categories in the PFSH.
Note: The Chief Complaint and History of the Present Illness must be performed by the practitioner and not by auxiliary personnel.
KEY COMPONENT 2: Examination
The Examination requirements are shown in Figure 1. Each bullet identifies an element that the practitioner must perform if that element is to be counted toward the level of the examination. No substitutions are allowed — you cannot take elements from other single organ systems and count them as eye examination elements. A total of 14 elements are identified by a bullet. At the highest level, all 14 have to be performed.
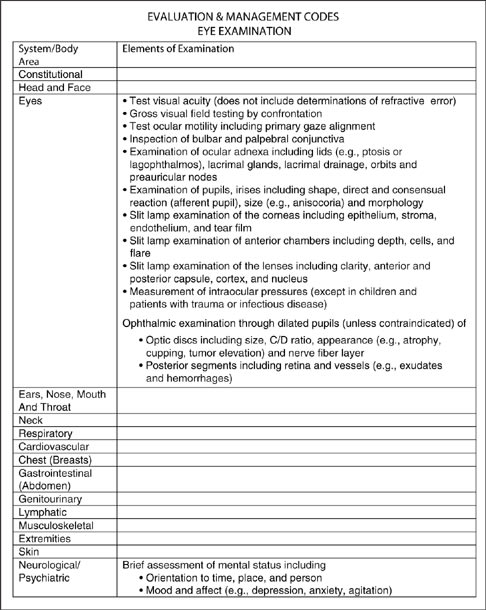
Figure 1 shows eye examination requirements for E/M codes.
At the bottom of the chart, you will find the leveling of the examination based on the number of elements performed and documented.
Here are some of the documentation problems I frequently encounter when auditing:
► Confrontation visual fields not addressed; if not done — state the reason.
► Primary gaze alignment is not "versions full" — you must address the primary gaze measurement.
► No reason given when intraocular pressure (IOP) is not measured.
► Pupils not dilated, and the two elements (optic nerve and posterior segment) are still being counted toward the level of the exam — with no explanation as to why. It has to be a medical contraindication — not that it's "a sunny day."
► Neurological/Psychiatric elements missing.
► Dilating drops not listed in the chart.
► Failure to check off normals for each eye, particularly when there is a problem in the other eye.
► Failure to describe the abnormality.
► Failure to perform all 14 elements. You cannot count an extended ophthalmoscopy as the basic elements of optic disc and posterior segment and also as the separate diagnostic test, extended ophthalmoscopy.
Note: Any element you are applying as an element performed when you select the level of the examination must be performed by the practitioner and not auxiliary personnel.
KEY COMPONENT 3: Medical Decision Making
Medical Decision Making is the most difficult of the three key components in E/M coding to master, chiefly because it's less quantitated than the other two key components — History and Examination. In its simplest form, Medical Decision Making is one of four adjectives — straightforward, low, moderate and high. It's rather intuitive — acute glaucoma is best described as high, whereas conjunctivitis is best described as low.
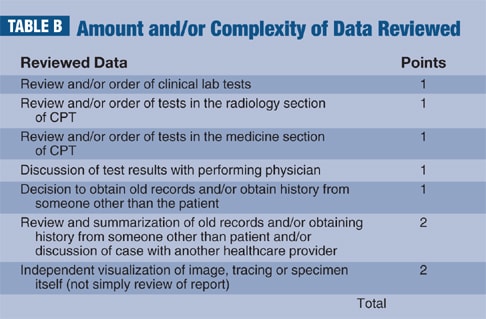
These are the four categories of Medical Decision Making: Straightforward, Low Complexity, Moderate Complexity and High Complexity. The complex method used for determining the level of Medical Decision Making is given (see Figure 2) based on those used by Medicare as audit guidelines. The selection of the proper category for the encount-er you are coding is calculated using Tables A, B and C.
One of the most troublesome tasks seems to be defining chronic illnesses.
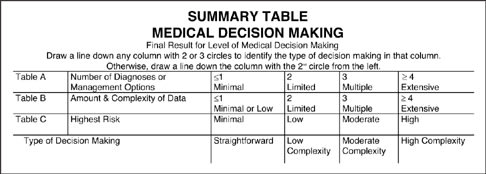
Figure 2. Medical Decision Making
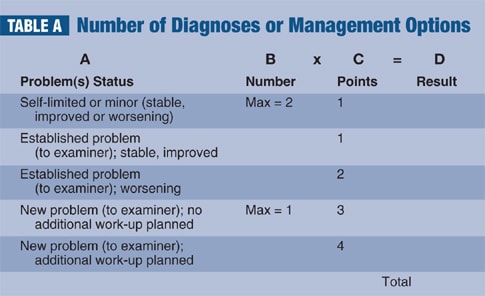
Chronic illness selection. The chronic illnesses should be ones that are diagnosed on the initial encounter or are being treated by the practitioner for follow-up examinations, such as glaucoma or a follow-up corneal abrasion. Incidental problems should not be counted just to enhance the level of risk. The level is also influenced by the state of the illness — whether it's stable, improving or worsening. A stable glaucoma would be low risk; a glaucoma that is not in control and requires change of medicine would be moderate risk. A patient presenting with acute glaucoma is considered high risk.
Management options. What is meant by "risk factors" isn't what a risk management agent would define as risk factors. Here, risk factors can be defined as the likelihood or probability that complications or unfavorable outcomes would occur with a given surgery with a given patient.
This is not to be confused with the fact that there are "risks" inherent in all surgeries, but rather the likelihood that this patient has a greater chance than average of not doing well. Thus, a patient with a standard cataract who is scheduled for surgery would fall into the moderate risk category (elective major surgery with no identified risk factors), whereas a patient who previously lost an eye secondary to an expulsive hemorrhage during cataract surgery and who also has had glaucoma surgery in the remaining eye, complicated by a severe chronic uveitis, would be in the high risk category (elective major surgery with identified risk factors) when that patient is scheduled to have an operation on the second eye.
When selecting the level of risk, think outcomes. What is the chance/likelihood that this patient will or will not have a good result? Keep in mind you are coding for that particular office visit/consultation.
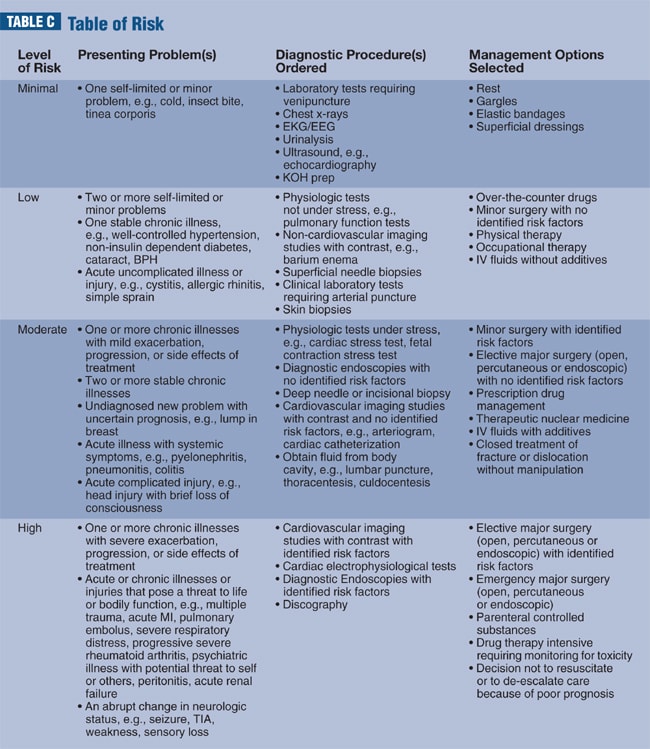
Note: Please pay close attention to the Table of Risk. This is the only one sanctioned by CMS. The word "referral" does not appear under any of the management options. You cannot claim any credit for referring the patient out in the Table of Risk.
The secret to proper chart documentation
The secret of facilitating proper chart documentation is a good forced entry chart. A version of my chart is presented here for your use (See "Figure 3," page 70). A similar version can be downloaded from my web site www.RivaLeeAsbell.com). When using a chart such as this, all elements of the history and examination must be checked off as being either negative or positive and normal or abnormal. Do not use squiggly lines. This is the first step to electronic medical records — all of which are based on this system. It's easy and fast and enables you to access all levels of coding.
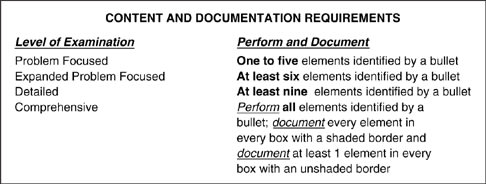
Figure 3. Shown is an example of a forced entry chart.
Pearls and pitfalls
When using E/M codes, be aware of the following:
► There is only one Table of Risk, and that is the generic Table of Risk to be used by all specialties. There is no ophthalmology Table of Risk sanctioned by Medicare. Note that the word "referral" does not appear in the document. You do not receive credit for referring a patient.
► Note the parenthetical comment "to the examiner" in Table A. This refers to the examiner and not the practice.
► When coding encounters for established patients, be sure to use both Table A and Table C.
► Requesting a consultation is not an activity that can be counted under Amount and Complexity of Data.
► The audit forms are the basis for audit sheets for Medicare. You, as the practitioner, should use them for your own internal self audits.
► Chief complaint and HPI technically are to be performed by you and you alone. You must perform or repeat any element that is counted in determining the level of the examination.
Next month (February 2009 issue), we'll discuss the Eye Codes. OM
CPT codes copyrighted 2008 American Medical Association.
| Riva Lee Asbell, a specialist in ophthalmic reimbursement consulting, can be contacted at www.rivaleeasbell.com. |