


CASE STUDY
When It's More Than Dry Eye
The case of an Iraqi war veteran who can't tolerate contact lenses or punctal plugs.

Thomas P. Kislan, O.D., Hazelton, Pa.
In those cases of moderate to severe dry eye disease or dysfunctional tear syndrome (DTS), you may consider a treatment plan that includes punctal occlusion. However, the following case study demonstrates that if you implant punctual plugs before you suppress DTS-related inflammation and lid disease, inflammatory mediators remain on the ocular surface, thereby exacerbating the debilitating symptoms associated with this syndrome and preventing tear drainage.
Back from Iraq
A 26-year-old male patient presented complaining of discomfort when he tried to wear contact lenses, which he hoped would replace "thick-lens spectacles." The patient, a +4.00D hyperope, recently returned from military service in Iraq. He said that during his tour of duty, he experienced scratchy, gritty, blurry vision when he attempted to wear contact lenses. He attributed these symptoms to the arid climate of the Middle East.
Upon his return to the United States, the patient explained that immediately after contact lens insertion, he would experience intensely painful foreign-body sensation that he was able to relieve upon contact lens removal. Prior to military service, the Iraqi war veteran said he'd worn contact lenses for three years without issue.


The patient presented with lid margin telangiectasia (above) and meibomian gland inflammation.
Further, he said that five days before his visit to our office, he visited a local corneal specialist who had inserted punctual plugs in the veteran's eyes. The patient said his discomfort increased after plug insertion and that as a result, he chose not to return to the physician.
The examination
Upon examination, best-corrected visual acuity (BCVA) was 20/30 O.D. and 20/25 O.S. We noted corneal dryness and lid disease, which a Schirmer score of 3mm O.D. and 4mm O.S. confirmed. Further, instantaneous tear break-up time (TBUT) O.U. and fluorescein staining revealed coalesced central staining O.U. Eyelid margin examination showed grade 2 injection; the lashes revealed grade 2 blepharitis; and the meibomian glands were blocked and difficult to express. We concluded that the patient had meibomitis and bordered on posterior blepharitis. Having the plugs inserted (in the presence of lid disease and inflammation) retained exotoxins from the staphylococcus aureus on the lids and cornea.

Evaluation of tear meniscus shows that build up of bacteria results in frothing of the tears.
The treatment plan
We removed the plugs, recommended lid scrubs and warm compresses and started the patient on cyclosporine ophthalmic emulsion 0.05% (Restasis, Allergan) b.i.d. for permanent management of DTS-related inflammation. We added an interim topical steroid and an oral antibiotic (doxycycline 100mg b.i.d. for 30 days and 100mg q.d. for 60 days) to eradicate the lid disease.
In this case, our use of cyclosporine aimed to break the cycle of inflammation and tissue dysfunction. As inflammation decreases and function improves in the ocular surface and lacrimal glands, the tear film begins to normalize. Restoration of normal neural feedback allows the lacrimal glands to produce more normal aqueous tears than before and other important components of the tear film. As the quality of the tear film improves, its ability to help promote a healthier ocular surface also improves.
Follow-up
At the patient's eight-week follow-up visit, he'd made approximately 80% improvement. He said he felt significantly more comfortable, and his eyes showed a marked reduction in redness. We discontinued the topical steroid at this follow-up visit; though we had him continue the antibiotic for four more weeks. We added an artificial tear as needed, and we continued the cyclosporine.
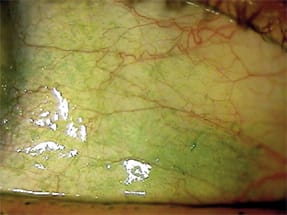
Conjunctival staining (grade 3) with lissamine green aids in lid disease diagnosis.
At this juncture in treatment, we explained to the patient that this was the appropriate time to insert punctual plugs because the lid disease and inflammation were almost completely gone. He agreed to try them again.
As we anticipated, the patient said he felt significantly better when we saw him at his next follow-up visit eight weeks later.
At his most recent visit, the patient showed enough improvement to be fit in a two-week soft contact lens (Extreme H20, Hydrogel Vision). To further quell his ocular dryness, we prescribed an oral supplement of absorbable omega-3 fish oil (LifeGuard Health) at a dosage of three caplets in the morning and evening (a total of four grams daily). The patient remains on cyclosporine b.i.d., and we plan to have him continue with this topical antiinflammatory drug indefinitely.
Cyclosporine doesn't eliminate factors that contribute to DTS, such as hormonal imbalance, causative primary disease or environmental exposure. This suggests that you should regard it as a long-term-to-permanent therapy.
Because DTS patients tend to be so uncomfortable when they present, it's important you discuss realistic expectations when prescribing cyclosporine. Thus, inform patients that improvement will be gradual; three to six months of therapy is typically required before they'll achieve the drug's maximum benefit. After one month, patients begin to notice reduced symptoms; at three months, key DTS signs continue to improve; and at six months, significant improvement in signs and symptoms is the norm. Continued therapy is necessary to maintain this improvement. Clinical tests with earlier, non-marketed ophthalmic formulations of cyclosporine have shown that if a patient discontinued therapy, their disease eventually returned to baseline levels of signs and symptoms.
Our patient's lid disease triggered his DTS. Addressing this with doxycycline and long-term omega-3 supplementation worked to alleviate the systemic condition that was exacerbating his ocular surface disease. Lid disease tends to wax and wane in patients such as this one who are fair complected and exhibit the signs of mild rosacea. To ensure that the rosacea doesn't progress, you, along with a dermatologist, should closely monitor these patients. I've found that cyclosporine helps keep the inflammatory cycle on the ocular surface in check nicely.
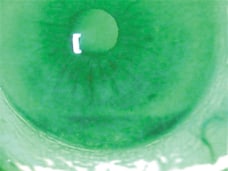
Tear break-up time also provides important information regarding dysfunctional tear syndrome diagnosis and treatment. (This patient's T-BUT score: 6.)
Conclusion
This case illustrates the importance of achieving and maintaining improvements in DTS-related inflammation and lid health before punctual occlusion.
One year ago, this patient was fighting a war as well as his own personal battle against debilitating eyelid disease. Today he's a student with a promising future as an emergency medical technician (EMT) who wears contact lenses comfortably. OM
Dr. Kislan is the medical director of Hazelton Eye Specialists, Stroudsburg Eye Associates and the Dry Eye Clinic of Northeastern Pennsylvania.