


optic disc elevation
Diagnosis and Management of Optic Disc Elevation
Making the right diagnosis can help avoid needless tests while saving lives and vision.
SHELDON H. KREDA, O.D., F.A.A.O.
Lauderhill, Fla.
The differential diagnosis of optic nerve head (ONH) elevation can make the difference between putting a patient through needless, expensive, risky tests and providing him with timely, life-saving treatment. The decision to order further tests rests upon the optometrist's confidence in the diagnosis, coupled with the relative risk of performing additional tests vs. the consequence of misdiagnosis.
Here, I provide methods to assist you in the differential diagnosis between benign disc elevations and those that have more insidious implications.
Understanding elevation
Disc elevation is not always due to edema, and disc edema is not always due to increased intracranial pressure (ICP). Therefore, disc elevation comes in three flavors: true disc edema with-out intracranial hypertension (ICH), papilledema and pseudopapilledema.
Optic disc edema results from compression, infection, infiltration, inflammation, demyelinating disease or reduced perfusion to the nerve. These conditions slow normal axoplasmic flow, resulting in an accumulation of intracellular fluids within the ONH.
Papilledema is a specific case of optic disc edema secondary to ICP. The ONH becomes engorged and swollen when cerebral edema spreads along the common meningeal sheaths of the brain and optic nerve.

Shown are Paton's lines. Note circumferential retinal folds temporal to swollen disc.
True papilledema signals ICH, a potentially life-threatening condition. There are no visual field defects associated with papilledema in early stages. As this condition progresses, there is gradual vision loss. When it reaches the chronic stage, there is peripheral constriction and nerve fiber bundle defects similar to glaucoma. If left untreated, papilledema can lead to optic atrophy and permanent loss of vision.
Pseudopapilledema has the appearance of disc swelling, but it has another, typically benign etiology. It may be congenital or due to ONH drusen. Pseudopapilledema often requires no treatment, as this frequently represents only a normal physical variation.
Causes
The causes of optic disc swelling not due to ICP include:
► Orbital tumors (motility defects, proptosis).
► Hypertension (accompanied by other obvious retinal signs).
► Papillitis: inflammatory, infiltrative and infective conditions that cause true disc edema (not due to ICH). Vision loss is an obvious distinction. Typically it's unilateral with an accompanying vitritis (red-green color defects).
► Papillophlebitis: mild visual loss and disc swelling in a young, healthy patient.
► Central retinal vein occlusion: unilateral, associated with an acute loss of vision.
► Diabetic papillopathy: disc edema with minimal visual loss, resolves spontaneously.
► Graves' ophthalmopathy: may include thyroid dysfunction, lid lag, proptosis and ICP.
Causes of pseudopapilledema include:
► Oblique insertion of the ONH.
► Small (heaped up) ONH (hyperopia).
► Myelinated nerve fibers.
► Buried disc drusen: swelling of the ONH from infiltration by hyaline bodies, which can be associated with visual field defects or afferent pupillary defect.
► Remnants of the hyaloid canal.
Ophthalmoscopic evaluation
The first step in evaluating any elevation of the optic nerve is to determine whether there is true disc edema or only pseudopapilledema. Papilledema and pseudopapilledema have no visual symptoms, and these patients usually present on routine exams.
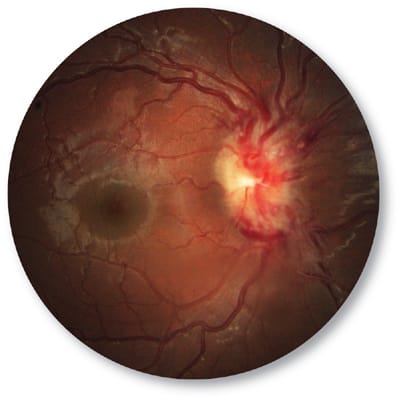
True papilledema (shown above) signals intracranial hypertension (ICH), a potentially life-threatening condition.
A careful ophthalmoscopic exam may be all that is needed to make the distinction. Papilledema is bilateral, while pseudopapilledema can be unilateral or bilateral. Although papilledema may appear asymmetric, a single apparent swollen disc in the presence of a normal contralateral ONH would not be papilledema. Swelling in true papilledema always begins on the nasal margin as opposed to the central elevation seen with pseudopapilledema. Papilledema typically develops slowly, but rapid progression can occur within hours for cases of subarachnoid hemorrhage.
With papilledema, the distinctive ophthalmoscopic appearance includes:
► Hyperemia.
► Dilatation of superficial ONH vessels.
► Flame-shaped hemorrhages and cotton wool spots.
► Paton's lines: circumferential retinal folds that surround the disc (usually temporal).
► Optociliary shunt vessels (seen in cup).
► Retention of optic cup until late in the disease.
► Surface telangiectatic vessels.
► Venous congestion.
► As noted above, swelling always begins on the nasal margin.
In the progressive stages of edema seen with papilledema, you may observe:
► Early: a pathologic "C"- shaped halo surrounding the disc.
► A circumferential halo.
► Edema obscuring major blood vessels as they leave the disc.
► Edema covering blood vessels on the disc.
With pseudopapilledema, the distinctive ophthalmoscopic appearance includes:
► Yellow appearance of disc (or mildly pale).
► Absent or small optic cup.
► No venous congestion.
► Spontaneous venous pulse (SVP)—though if absent does not rule out pseudopapilledema.
► Swelling begins centrally.
► Anomalous vessels on the disc, both tortuous and trifurcation (vessels that branch before they reach the retina).
► Pigmentary loss at the disc makes choroidal vessels more visible.
► No halo of edema.
► Major vessels are not covered (remain visible).
► Blood vessels follow the contour of the elevated edge (as opposed to being covered by elevation).
► The high point of elevation is central.
Imaging assistance
Clinicians may use imaging devices — B-scan ultrasound, fluorescein angiogram (FA), stereo color photos and optical coherence tomography (OCT) — to assist in the differential diagnosis of ONH elevation.
With B-scan ultrasound, drusen appear highly reflective, and papilledema shows a distended optic nerve sheath.
In FA, late dye leakage beyond the disc margin indicates papilledema. In addition, drusen may autofluoresce, and you may observe an increased number of capillaries and venous congestion with papilledema. No leakage of dye would indicate pseudopapilledema and may spare the patient from neuroimaging.
With stereo color photography, you may monitor and follow changes, such as small hemorrhages of the retinal nerve fiber layer (RNFL) or disc hyperemia.
OCT provides a quantifiable view of disc elevation that can play a role in detection, along with assessment of progression or resolution of pathology. Disc edema as imaged by OCT shows substantial elevation due to tissue thickening and fluid accumulation viewed as a dark (hollow) space within the ONH in conjunction with peripapillary RNFL thickening.
Equating OCT findings with the patient's visual fields is valuable for the follow-up of papilledema. OCT does not help to clearly differentiate papilledema (especially if it's mild), pseudopapilledema or a congenital elevation of the ONH, since it only reveals increased thickness. The exception: the ability of OCT to detect the presence of ONH drusen, especially when undetectable by the ophthalmoscopic appearance.
Although OCT will not prevent the need to perform neuroimaging tests, for patients afflicted with a more severe case of papilledema, measured thickness is often greater than that seen with pseudopapilledema and may lend support to the differential diagnosis. Because OCT is objective, noninvasive and reproducible, it can be an invaluable aid during follow-up to assess treatment and detect recurrences.
Other diagnostic tips
You can best observe drusen using a direct ophthalmoscope or slit lamp that has a fundus lens. ONH drusen can best be seen using indirect illumination. Use a cobalt blue filter to observe autofluorescence.
When testing for ONH elevation, look for concomitant symptoms of elevated intracranial pressure, which include headache, nausea, vomiting, diplopia and amaurosis fugax (transient loss of vision lasting only a few seconds due to changes in posture). Include in your examination:
► Measurement of blood pressure.
► A check for neck tenderness and stiffness.
► A check for temporal artery tenderness.
► Ask about pain in and around eyes when checking rotations.
► A test for an afferent pupillary defect. (A positive finding indicates an ocular etiology rather than ICP.
► Observation and documentation of the presence of a spontaneous venous pulse (SVP). Although SVP is absent in a large percentage of normals, its presence would rule out elevated intracranial pressure.
If disc edema is found, the following laboratory tests are recommended:
► Sedimentation rate and C-reactive protein, which can rule out temporal arteritis.
► White blood count, which can rule out infection and leukemic infiltration.
► Computerized Axial Tomography (CAT) or magnetic resonance image (MRI) scan to rule out compressive lesion.
► Cerebrospinal fluid (CSF) examination to rule out meningitis, tumor or hemorrhage (only after a scan has ruled out a compressive lesion).
When you suspect papilledema, schedule a consultation with a neurologist, even if there are no neurologic signs or hypertension. Order a CAT scan with and without contrast (preferred to view acute intracranial bleeding). If the CAT scan is inconclusive, order an MRI and MRI angiography.
After the referral
Once you decide to refer, you must remain part of a multidisciplinary approach that encourages open communication between doctors. Guide the neurologist and neurosurgeon by carefully monitoring the patient's visual acuity and color vision. Visual field testing can prevent vision loss by detecting peripheral field constriction — a more sensitive measure of progression to the chronic and atrophic stages than is the ophthalmoscopic appearance. Field loss signals irreversible damage to the optic nerve, and you must alert the neurologist of the urgency to alter treatment. Patients who have early and established papilledema can recover full visual fields and vision within days to weeks given timely, appropriate treatment. Still, residual disc elevation may remain indefinitely.
The optometrist is critical
Your role is pivotal to differentiating optic neuritis and pseudopapilledema from true papilledema. Too conservative an approach withholds treatment for a potentially life-threatening condition. On the other hand, many optic nerve disorders are misdiagnosed as papilledema. This subjects patients to needless testing that carries high cost and potential risk. Carefully distinguish these disorders, and either treat accordingly or refer to the appropriate specialist. OM

|
Dr. Kreda practices in a primary care setting in Lauderhill, Fla. He's a frequent lecturer and author. You can e-mail him at EyeRx@comcast.net. |