


IOLs
Understanding the Latest IOL Technology
By understanding advances in design, you can match your patient with the best lens.
JUSTIN HOLT, O.D., Ogden, Utah
The technology of premium intraocular lenses (IOLs) has been one of the most advanced and successful in eye care through the last five years. In contrast to previous years, patients now have a host of lenses available to customize their surgical outcome to accommodate their particular lifestyles, careers and hobbies. Today's eyecare professionals need to be aware of available lens options in order to provide patients with the surgical outcomes they desire. Optometry was built on optics and the art of refraction, making optometrists more than qualified to discuss the refractive characteristics of particular IOLs, including which would best suit the patient's lifestyle.
More than a cataract patient
When discussing premium IOLs, realize that the patient is now not only a cataract patient but also a refractive surgery patient. Your goal for these patients is to enable them to obtain as much freedom from glasses as possible with the least amount of side effects. That being said, there is no "perfect" IOL — one size does not fit all. The patient who regularly drives at night has different needs than the patient who performs a lot of near point tasks. We need to choose the lens that best suits the patient's needs.

Having previously removed the cataract, the folded IOL is injected through the temporal incision. 
Once in the eye, the IOL begins to slowly unfold on its own. 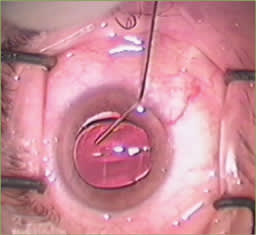
As the IOL unfolds completely, it is maneuvered into its final position. |
Aspheric IOLs
In nature, the cornea induces positive spherical aberration, which is balanced by negative spherical aberration in the crystalline lens. Spherical IOLs induce positive spherical aberration, adding further to the positive spherical aberration of the cornea.
Optically speaking, spherical aberration occurs when light rays are over-refracted at the periphery of a lens system, resulting in a region of defocused light, which can decrease image quality. Aspheric optics align the light rays to compensate for positive corneal spherical aberration, resulting in enhanced image quality. The most recent aspheric IOL technologies are designed with negative spherical aberration to offset the average positive spherical aberration of the cornea.
Aspheric IOLs have been shown to improve mesopic contrast sensitivity at a clinical level. While studies have concluded that patients, particularly those in their 60s or older, may not be able to appreciate this benefit, aspheric IOLs continue to grow in popularity. These lenses are often limited to patients who have a low degree of corneal astigmatism. They can be used in patients who have high levels of cylinder. But, without correction of their astigmatism, their uncorrected acuity will of course still be limited — in theory, they would still receive the optical benefits of the aspheric optic. These patients would require either surgical astigmatism correction (limbal relaxing incision [LRI] or LASIK) or have to simply wear glasses. As such, most surgeons use aspheric optics for all monofocal candidates unless the patient requires an unusual power not available in an aspheric design.
The aspheric IOLs include the SofPort Advanced Optics (Bausch & Lomb), the AcrySof SN60WF (Alcon) and the Tecnis Z9000 (Abbott Medical Optics).
Toric IOLs
Surgeons address astigmatism in cataract patients with a number of options, including toric IOLs, LRIs, spectacles, LASIK or a combination of these. Treatment can depend on the amount of astigmatism. For example, those patients having more than 3.0D of astigmatism may be corrected with a toric IOL and subsequent LASIK or LRIs.
Previous toric IOLs had a tendency to rotate, making postoperative refractive outcome unpredictable. Recently, the Food and Drug Administration (FDA) approved the AcrySof Toric (Alcon). This latest version of a toric IOL improved both rotational stability and significantly improved uncorrected distance visual acuity over previous toric IOLs. It currently is available with effective cylinder power corrections of 1.0, 1.5. and 2.0.
Presbyopia correcting IOLs
Two technologies exist to attempt to provide cataract patients with freedom from reading glasses: accommodating IOLs and multifocal IOLs. Currently, the only truly accommodating IOL available in the U.S. is the Crystalens 5.0 (Bausch & Lomb). The lens features a hinged plate-haptic with a relatively small silicone optic. When the patient attempts to accommodate, the ciliary body contracts, and the tension on the capsular bag diminishes. The increased pressure within the vitreous body then allows the lens to vault forward at the hinges, resulting in near focus.
The latest version, the Crystalens — 5.0 HD — has a larger plate-haptic allowing for greater movement and thus greater range of accommodation. It also has an enlarged optic zone (4.5mm to 5.0mm) and incorporates a unique change in the central asphericity of the optic that produces an optic optimized for reading. (A limitation of the earlier version of the Crystalens is that patients felt their near vision was limited.) Also, the Crystalens provides excellent vision at distance and intermediate range.
The AcrySof ReSTOR (Alcon), ReZoom (Abbott Medical Optics), and Tecnis (Abbott Medical Optics) multifocals provide simultaneous vision. These lenses are based on refractive and diffractive optics, respectively. Light from multiple focal planes is simultaneously being focused on the retina at any one time. These multiple planes will cause light scatter, and patients may report halos at night, which will require some neuroadaptation on the patient's part. Similar to patients adapting to monovision, this can take anywhere from a few minutes to six months.
In cases in which patients are very concerned about halos and glare, I use a -2.50D loose lens over each eye and demonstrate what their vision would be at near, if they had chosen a monofocal lens. This often reassures them that they made the right choice, and that the small amount of glare at night isn't as bothersome as their near vision would be with a monofocal lens.
Built on the platform of a first-generation multifocal IOL (the Array), the ReZoom further improved on the Array's design by utilizing five optical zones proportioned to provide good visual function across a range of distances in varying light conditions. The center of the optic is distance-dominant; the second zone provides near-dominant vision. The other four concentric refractive zones create true multifocal vision. Zones 1, 3 and 5 are distance-dominant, while zones 2 and 4 are near-dominant. An aspheric transition between zones provides balanced intermediate vision. In addition to this, the size of the rings has been altered in proportion to those used in the design of the Array lens.
These modifications have greatly decreased the degree of dysphotopsia. The ReZoom typically provides very good distance and intermediate vision, and typical near vision tends to be around J2. Despite the add being 3.5D, the effective add at the corneal plane ends up being about a 2.25D.
AcrSof ReSTOR is a diffractive-refractive optic IOL that uses a mathematically derived image enhancement algorithm called apodization. Apodization gradually blends the diffractive step heights, effectively managing the light that is delivered to the retina, thus improving vision quality while at the same time minimizing visual disturbances. Balanced use of optical power, number of diffractive rings, step height and ring width are factors that afford enhanced contrast and image quality improvement. The AcrySof ReSTOR uses a 12-zone design, with the first ring at an elevation of 1.3 microns and tapering to a 0.2 micron 12th ring for effectively delivering slightly over 3.00D at the corneal plane. Beyond the apodized diffractive center lies the peripheral refractive zone of the IOL. The refractive region that surrounds the apodized region is utilized primarily when pupils are dilated, as in night driving; light then is refracted to focus distance objects. This provides very good vision regardless of pupil size.
Alcon recently gained approval for the AcrySof IQ ReSTOR IOL +3.0. It utilizes the existing ReSTOR platform with identical asphericity, nine diffractive steps vs. 12 diffractive steps and slightly wider step spacing to modify the add power. The add power was modified from +4.0D to +3.0D. This changes the effective add from 3.0 to 2.5.
The Tecnis Multifocal IOL (Abbott Medical Optics) is the latest IOL to gain FDA approval. It is a non-apodized, fully diffractive aspheric lens that corrects the two highest-order aberrations: spherical and chromatic. Diffractive rings on its posterior surface provide patients with a near and a distant focus. The rings start very close to the optic's center continuing out toward the periphery. As a result, its multifocal effect is completely independent of pupil size. Even in the presence of relatively small pupils, this IOL provides excellent near vision.
The Tecnis Multifocal IOL improves contrast by reducing higher-order aberrations compared with a normal monofocal optic. This comes from incorporating two optical principles: multifocal optics and an aspheric anterior surface.
Phakic IOLs
Candidates for phakic IOLs are unique: Typically, they do not have symptomatic cataracts, are younger than age 45, have large amounts of myopia and due to the degree of myopia and/or thin corneas, are not LASIK candidates.
The FDA approved the Visian Implantable Collamer Lens (ICL) (STAAR Surgical) in 2005. The Visian ICL is a foldable, posterior chamber, ciliary sulcus-based lens. Previous phakic IOLs were not foldable, required much larger incisions and needed to be closed with sutures. The Visian ICL is more aesthetically pleasing than its predecessor post-surgically, as the lens is invisible in the eye. It is approved to treat myopia from 3.00D to 20.00D and less than 2.0D of astigmatism.
A very nice feature of phakic IOLs: Patients maintain their natural level of accommodative focus postoperatively, and if necessary or when a pseudo-phakic IOL is needed, the ICL is easily removable. However, unlike other IOL implantations, phakic IOLs have the unlikely but added risk of cataract formation.
Remember to appropriately screen, educate on the available technology and counsel IOL patients. If you and the patient truly understand each other regarding the patient's postoperative expectation and the limitations of the current IOL technologies, then the patient will do well. OM
Optometric Management thanks Skip Nichamin, M.D., of Brookville, Pa, for reviewing this article.

|
Dr. Holt is in group practice at the Mount Ogden Eye Center and Bountiful Hills Eye Center. He completed a residency at the University of Utah Moran Eye Center and Veterans Hospital. He can be reached at jchod5150@yahoo.com. |