


keratoconus
A Clear Vision for KC Patients in Your Practice
How to succeed in managing (and delighting) patients who have keratoconus.
CHRISTIAN P. GUIER, O.D., F.A.A.O. Jacksonsville, Fla.
In optometry, little is as rewarding as successfully fitting a complex keratoconic patient with a uniquely designed specialty contact lens. Similarly, nothing may be more challenging than achieving a comfortable, stable fit that offers reproducibly clear visual function.
Understanding KC
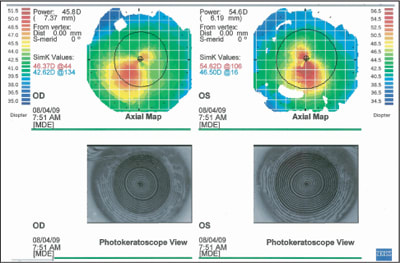
Keratoconus (KC) is characterized as a non-inflammatory condition affecting the rigidity of the corneal tissues. Progressive corneal thinning results in paracentral ectasia and irregular astigmatism. These findings are usually bilateral yet often markedly asymmetric. Topographic data distinguishes subsets of ectatic configurations. Estimates suggest that an oval distortion displaced inferior temporally characterizes the majority of KC. The nipple cone consists of an abrupt paracentral elevation that is readily evident upon physical exam of the eye. Pellucid marginal degeneration and keratoglobus are clinical rarities likely related to keratoconus. The characteristics of the type of KC significantly influence contact lens fitting options.

A large diameter semi-scleral GP contact lens may be necessary for significant corneal irregularities.
Functional changes associated with KC include blurred vision, glare, distortions and monocular diplopia, or polyopia, at distance and near. KC incidence in the general population is estimated at 0.15% to 0.6%. Onset and prognosis are variable. But, studies suggest that males present with the condition earlier than females, often as early as their mid-teen years. Dynamic alterations in corneal contour and refractive error are seen up to the fourth decade of life. Significant change in these areas after that time is rare. The rate of change is unpredictable, but young patients are thought to progress more rapidly than older KC patients.
The poorly predictable corneal contours require unique fitting curvatures to offer both stability and comfort. Surgical correction may be considered for those who have an advanced condition and are contact lens intolerant or have limited vision due to apical scarring. Corneal cross-linking procedures offer the potential to stabilize emerging ectasias. While the use of Intacs intrastromal corneal ring segments for KC has increased significantly through the last few years, penetrating keratoplasty (PK) remains the most common surgical intervention for visual rehabilitation. In fact, one in five patients who have moderate to severe KC will require PK in their lifetime. KC patients who have not required PK by age 40 rarely go on to need this procedure in the future.
Grading KC
While a variety of grading criteria have been proposed to characterize the extent of the physical and functional compromises due to KC, the most straightforward method identifies KC as mild, moderate and advanced. In mild KC few, if any external signs are present. When patients report deteriorating vision associated with progressive myopic refractive error — especially in the presence of significant astigmatic correction — be suspicious. Order ker-atometry or videokeratography to look for evidence of topographic irregularities, such as inferior or central corneal steepening. Correction for mild KC includes spectacles, toric soft contact lenses and standard GP contact lenses.
As KC progresses to moderate and advanced levels, the external/corneal signs are much less difficult to discern. Bold corneal nerves, Vogt's striae and/or Fleischer ring may be evident on slit lamp examination. GP contact lenses are the main stay of moderate to advanced keratoconic correction. Videokeratography offers a detailed quantitative analysis of the KC characteristics. If the diagnosis is in doubt, corneal pachymetry demonstrates the apical thinning associated with KC. You may see thin pachymetry in non-KC eyes, however the rate of change from the thin apex to the relatively normal peripheral cornea is much more abrupt in KC.

A hybrid design may offer improved centration of the GP optics.

Apical touch is bound to occur with moderate and advanced KC.
Frustrated keratoconic patients present to all modes of optometric practice. Spend a significant portion of the initial exam establishing the patient's current status and needs. Once you establish a diagnosis of KC, discuss corrective options and anticipated outcomes with the patient prior to initiating the fitting process. Emphasize that the professional services necessary to achieve success are more complex and time consuming than fitting standard contact lens technology on non-KC eyes. This is so the patient understands and is prepared for the cost differential.
If KC is the initial diagnosis, thoroughly educate the patient about the condition. Include discussion regarding the diagnostic tests used to measure the corneal anatomy, how this varies relative to “normal,” how KC has affected visual function and what changes might occur in the future. Outline treatment options. If you have the opportunity to meet the patient's needs with spectacles or soft (toric) contact lenses, proceed with the routine examination.
Beyond the first tier
When KC patients do not achieve significant visual improvement with the first tier of options, perform a diagnostic evaluation of visual performance with a tricurve or KC-specific GP contact lens. This method confirms the patient's best-corrected visual acuity while simultaneously demonstrating the benefits of specialty contact lenses to the patient. Tell the patient to be prepared to pursue more advanced corrective options as KC progresses. Advise patients of the technologies you have embraced for correction and what the fitting process might entail.
Patients who have a known history of KC — particularly if moderate or advanced — are likely to appreciate the complexities of their condition. Explain to the patient his current status of KC and measured changes through time. If it is necessary to consider refitting contact lenses, state to the patient how updated designs would aid vision, comfort, stability and ocular health.
Patients often appreciate learning of support and other resources. For instance, the American Optometric Association offers written and animated patient education on KC at www.aoa.org. Also, the National Eye Institute's Web site (www.nei.nih.gov) offers patient information and an over-view of government-funded research. The National Keratoconus Foundation's Web site (www.nkcf.org) provides education and a range of support.

A steep base curve and smaller diameter allows great clearance but will decenter inferiorly over the apex.
Optimizing your practice
Competent and progressive contact lens fitting for KC likely requires additional chair time and office organization. Several basic concepts will help you, your staff and patients conserve time outlay. My practice, for instance, has developed a team approach to KC management to ensure that staff members have dedicated responsibilities. Upon scheduling the initial appointment, the front office staff identifies known-KC patients. This allows these new or complex patients to be placed in slots with adequate time allotment. The front office staff reminds new patients to obtain and bring previous records for review. The staff include “flags” in the patient's file, which alert technicians to perform special testing, such as keratometry and topography. The technician completes these tests before the patient sees the doctor. Similarly, train technicians to appreciate the subtle symptoms of early KC. Patients who report monocular diplopia at any time should undergo diagnostic topography regardless of their stated interest in contact lenses.
At the initial exam, a careful history details real or perceived progression and a history of corrective measures, including previous contact lens experience. The refraction and thorough slit lamp exam dictates the best course of action. Have your contact lens technician sit in on the conversation as the fitting proceeds. Include all members of the team at the point of initiating treatment. This reduces redundancies and gives the patient confidence that the team is working in unison. As other team members continue their responsibilities, the doctor is now free to work with patients in adjacent rooms.
Stock a variety of lenses
It is crucial that a variety of diagnostic contact lenses be available in your office. If you stock a soft toric contact lens that offers acceptable vision and stability, then the patient will enjoy leaving the office with an adequate corrective option on the same day. For those who require KC-specific contact lenses, have a couple of design variations on hand, as no single design will equally address the unique characteristics of the differing morphologies.
For the fitting, incorporate a well-trained technician who is able to identify proper fitting characteristics. Use a “rapid fire” approach to allow placement of the initial diagnostic contact lens and step-wise adjustments, which are made based on fluorescein staining patterns and lens movement. Often, a short duration is necessary for the diagnostic contact lens to settle.
It's important to instill patient trust by counseling him regarding costs of services and materials, as well as the warranty period and follow-up interval, prior to ordering contact lenses. Again, in many instances, you may delegate over-refraction of the diagnostic contact lens. After the technician determines appropriate alignment, return to review all aspects of the initial fit with the patient.
Generate the KC contact lens orders on a timely basis. Custom-crafted specialty contact lens designs require both manufacturing and shipping time. Access to timely processing may bias the choice of the contact lens design or laboratory. Pre-schedule patients for follow-up appointments or defer scheduling until the ordered contact lenses have arrived. Timely follow-up ensures that patients remain highly motivated while preserving useable days within the lenses' warranty period.
At follow-up, the contact lens technician prepares the contact lenses in advance, fits the contact lenses and allows them to settle on the eye for an adequate time before measuring visual acuity. You then address the fit and function of these contact lenses prior to the patient undergoing lens placement, cleaning and storage training. Review with the patient all impressions, wear schedule recommendations, risk status and follow-up information. Consider issuing a business card so the patient has access to care should difficulties arise.
The extent and location of the KC apex can vary widely.
Routine follow-up
The subsequent follow-up appointment is often routine. The technician reviews the patient's assessment of comfort and function. The technician addresses straightforward difficulties — especially those associated with handling and care — prior to the practitioner's evaluation. The practitioner then addresses any deficiencies in fitting characteristics, which may require an additional diagnostic contact lens evaluation, a change in lens design or considering the addition of a silicone hydrogel soft contact lens as a piggyback carrier, all of which can be time consuming. More often, consultation with the laboratory that produced the contact lens would allow adjustments in contact lens design that address any of the fit concerns. Establish close relationships with lab professionals, as they routinely consider similar dilemmas and problem-solving scenarios and can be a tremendous resource.
Without a thorough accounting of lens cost, shipping, replacement and warranty periods, the potential for profitability is greatly diminished. Therefore, assign a staff member to order, sort and track specialty contact lenses. The individual performing these tasks must work hand-in-hand with the practitioner and the lead contact lens technician. If the lead contact lens technician also performs these duties, build a certain amount of administrative time into the schedule so that the technician can carefully tend to these accounts. Schedule this administrative time to minimize the potential for understaffing patient care.
Additional resources
Web-based programs allow you and your staff to familiarize yourselves with the latest contact lens options. High-quality webinars demonstrate special contact lens features presented in real time by expert presenters. Often, there is opportunity for an involved question and answer period. The Gas Permeable Lens Institute (www.gpli.info) offers a wide range of valuable information, including online symposia covering a variety of specialty topics. SynergEyes (at www.synergeyes.com) offers a listing of webinars.
Capture all appropriate fees
An expert fitter of complex contact lens technologies receives many patients by referral. As KC is a clearly defined medical condition, it's appropriate to bill consultation fees in addition to contact lens fitting fees, as long as you communicate properly with the referring doctor. Be prepared to compose a letter of medical necessity including a brief description of the diagnosis, current status, prognosis and treatment options. In addition, consider ancillary testing when billing. While corneal topography, photography and refraction are procedures that may influence the contact lens fitting, they also act as valuable documentation of the disease process. Therefore, ensure that follow-up visits address the medical status of the eye in addition to a contact lens specific evaluation.
With increasing familiarity with traditional contact lens options and the emergence of new contact lens designs, you can look forward to a streamlined process yielding great patient success. Managing the process is as challenging as managing the disease itself. Take care to schedule the patient for maximum efficiency, to incorporate a team approach to patient care and to monitor the many details involved in ordering specialty contact lenses. OM

|
Dr. Guier practices at the Mayo Clinic in Jacksonville, Fla. An assistant professor in Ophthalmology, Mayo School of Medicine, he received training at Nova Southeastern University and residency training at the Bascom Palmer Eye Institute, University of Miami. |