


Comanaging Patients with Retinal Disease
Staying involved in their care can be a win-win strategy for patients and optometrists, too.
By Desiree Ifft, Contributing Editor
Like most new ODs who are fresh out of optometry school, you'll probably want to use your education and training to provide the highest possible level of service to your patients by comanaging with cataract and refractive surgeons. What you may not realize is that you can accomplish the same goals by working closely with retina specialists as well. “There's no reason for a patient who has a retinal issue to stop seeing his primary eyecare provider,” says John Warren, OD, Racine, Wis. In fact, when an optometrist stays involved in the care of his patients with retinal disease, everyone benefits.
How Patients Benefit
“Patients have a certain level of comfort with their primary eyecare provider,” says Jeffry Gerson, OD, FAAO, Kansas City. “The more care patients can receive in this setting, the more comfortable they'll be. It's also likely to be more convenient.”
Dr. Warren agrees: “For example, let's say a patient has undergone surgery for retinal detachment and his IOP increases. If the patient can receive treatment for the elevated pressure from the optometrist, typically there's less of a wait for an appointment, less distance to travel and less time spent in an unfamiliar environment. Furthermore, no one knows the patient better than the primary eyecare provider. He's seen the patient many times, perhaps for years, and at the very least he has the patient's records. The optometrist knows details, such as what the patient's visual acuity has been, and understands the patient's apprehension level.” And, as Charles Brownlow, OD, FAAO, associate director of the American Optometric Association's Third Party Center, points out, “Primary care providers are simply in a position to notice more things about their patients. They're more likely to notice subtle, but potentially important signs, such as speech patterns, skin color and so on.” Direct relationships between optometrists and retina specialists also can eliminate duplication of services, Dr. Warren says. “If optometrists refer patients who require retinal treatment directly to retina specialists instead of to general ophthalmologists, patients can avoid an extra visit and exam. Patients have more efficient access to appropriate care.”
How Doctors Benefit
Efficient access to appropriate care is more important than ever for patients with age-related macular degeneration (AMD), now that anti-vascular endothelial growth factor (anti-VEGF) agents are available. The sooner the disease is diagnosed and treated with these drugs, the better the visual outcomes. This is one reason many retina specialists appreciate a direct relationship with optometrists. Retina specialists see patients sooner and, as a result, can provide treatment earlier.
Another reason retina specialists may welcome optometric co-operation is that it frees them to focus on their area of expertise, says David Way, OD, Spring, Texas. “They can treat the specific retinal condition and then return the patient to the optometrist for other aspects of eye care. In the case of a diabetes patient who also has a cataract, for example, the retinal surgeon can focus on the retinopathy treatment, while the optometrist deals with the cataract.” This would include informed communication with the cataract surgeon, for whom the patient's diabetes would be a major concern. Dr. Gerson elaborates: “Retina specialists are trained to perform surgery, so it's in their best interests to see patients who require posterior segment surgery.”
Forging professional relationships with retina specialists is advantageous for optometrists, too. “It enables us to provide better care, because we're fully aware of what procedures and treatments our patients have had and what medications they're taking,” Dr. Warren says. These relationships also allow optometrists to ensure patients are receiving a high level of overall care, “because we're providing it,” Dr. Gerson says, adding that this can be a practice-builder as well. “It helps us maintain and solidify our relationships with patients. It also helps generate referrals because it becomes clear to patients that ‘my eye doctor can take care of more than just eyeglasses.’”
Cataract vs. Retinal Comanagement
While cataract and retinal disease comanagement provide the same benefits for patients, optometrists cite a key difference in how eye care is typically shared with cataract surgeons and retina specialists. As Dr. Way explains, “The comanagement of patients with retinal disorders isn't necessarily traditional comanagement—as with cataract surgery.”
Here's why: The rules and regulations set forth by Medicare and most other major medical insurance carriers define what's known as a global surgery package for each surgical service. The allowable fee (ie, reimbursement) set for each global package includes specific preoperative care, the surgery itself and specific postoperative care. The carriers limit the length of the pre- and post-op periods. The length of the post-op period for major surgeries is 90 days. The length of the post-op period for minor surgeries can be either zero or 10 days.
Whenever a surgeon performs a procedure, he can choose to provide all of the post-op care or transfer primary responsibility for post-op care to another qualified provider (ie, an optometrist). Comanaging cataract surgeons commonly transfer care to the optometrist by the third day post-op, which is well within the global post-op period. Therefore, this type of comanagement is subject to all of the rules governing care provided in a global period. The rules cover all aspects of care, beginning with requiring a written explanation of who will provide care and for what length of time. They also cover what services are and aren't part of the package. Any services provided during the designated post-op period that are related to the surgery are included in the total allowable fee and therefore shouldn't be billed separately. Medicare and most other major medical carriers generally reimburse the surgeon 80%of the total allowable fee for providing pre-op and intrasurgical care. The provider to whom post-op care is transferred receives 20% of the total allowable fee.
In contrast to this traditional cataract surgery comanagement model, optometrists sharing patient care with retinal surgeons typically aren't doing so within a global surgical period. Rather, they're examining patients for signs and symptoms of retinal disease and closely monitoring them until treatment by a retina specialist becomes necessary. “The retina is a hyperspecialized part of the eye, and often the outcome of treatment determines whether additional treatment is needed immediately,” Dr. Way says. “For that reason, and because many retina treatments in use today are new, retina doctors often prefer to monitor patients themselves for the entire global period.” However, the surgeon keeps the optometrist informed of what was done, the results, and when the patient will be sent back to the optometrist for eye care that's not directly related to the surgical procedure. “It's more comanagement of the patient as a whole than comanagement of a specific retina treatment,” Dr. Warren explains. Retinal comanagement certainly could be handled in the same way as cataract comanagement, but that's not the norm at this time, Dr. Brownlow says. “Optometrists shouldn't be surprised if a retinal surgeon wants to keep a patient for the entire global period,” he says. “This is partly because so few ODs have broached the topic. It's unlikely a retinal surgeon will contact an optometrist and invite him to participate in patient care. It just doesn't happen. It didn't happen in cataract care, and it won't happen in retinal care unless optometrists make it known that they're willing and able to participate.”
Getting Started
Reaching out to nearby retina specialists is what Drs. Warren, Gerson and Way have done to forge close working relationships. “It's important to find a practice you're comfortable with, so you can be confident when referring patients,” Dr. Warren says.
The surgical practices must be amenable to optometric comanagement. Beyond that, they should be committed to ongoing and detailed communication with the referring doctor. Other criteria to consider include the services the surgical practice provides, its reputation among patients and if more than one specialist is available to ensure complete coverage. “Open conversations are key to determining what surgeons and optometrists expect from the relationship and what each is comfortable with,” Dr. Gerson says.
Drs. Warren, Gerson and Way also recommend that optometrists interested in retinal comanagement ask to shadow the specialist in the clinic for at least a few half days to see how the specialist examines patients and how disease processes and procedures are discussed. “You don't want to give patients a different understanding than what the retina doctor is giving them,” Dr. Way says. “You can see a wide array of conditions in a short amount of time and gain a better understanding for when surgery may be needed. Some treat certain conditions more conservatively or aggressively than others. In addition, spending time at the retina practice allows the surgeons to gain confidence in you. They may not know how well trained and well versed you are in retinal care until they see it for themselves.”
When to Refer
The majority of patients that optometrists comanage with retina specialists are those who've had treatment for or are at risk for developing neovascular AMD or diabetic retinopathy. According to Dr. Warren, any competent optometrist can detect the presence of these conditions. However, how far he wants to follow patients before referring them to a retina specialist for intervention varies. As Dr. Gerson explains, “You have to know your comfort level. Everyone's comfort level is different and that's OK. Some optometrists want to follow patients until they know surgery is required. Others may want to send patients with even mild pathology to the specialist right away and not be involved any further.”
The optometrists interviewed typically don't refer patients with early AMD unless signs of choroidal neovascularization (CNV) emerge. The signs include subretinal fluid or blood, retinal elevation, hard exudates, retinal pigment epithelium detachment or a sudden decrease in visual acuity. “Any signs of CNV necessitate fluorescein angiography by a retina specialist to confirm and determine whether treatment is indicated,” Dr. Warren explains. “If no sign of CNV is present, a retina specialist wouldn't do anything more than I'd do, which is to continue monitoring the patient.”Inthe meantime, Dr. Warren adds, he can counsel patients about the benefits of AREDS supplements for reducing the risk of AMD progression. He al so can help maximize vision for patients who've already undergone retinal procedures by educating them about low vision aids and treating conditions that further reduce visual acuity, such as dry eye.
The doctors follow similar protocols when caring for diabetes patients. They refer patients to a specialist based on the longstanding treatment criteria established by the DRS, ETDRS and DRVS clinical trials. These landmark trials provided guidelines that helped determine at what point in the course of diabetic retinopathy surgeons should apply laser treatment and vitrectomy to preserve vision.1–11
The trials also confirmed that laser photocoagulation reduces the risk of vision loss from clinically significant macular edema (CSME), which is defined as:
■ Retinal thickening at or within 500 μm of the center of the macula (Figures 1 and 2)
■ Hard exudates at or within 500 μm of the center of the macula if accompanied by thickening of the adjacent retina
■ An area or areas of retinal thickening at least 1 disc diame ter in size at least part of which is within 1 disc diameter of the center of the macula.
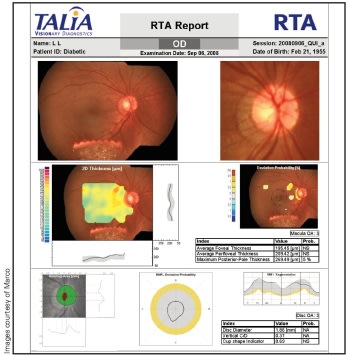
Figure 1. Based on established treatment criteria, focal or grid laser photocoagulation wouldn't be indicated for this diabetes patient. While retinal edema is present, it's not within 500μm of the foveal center.
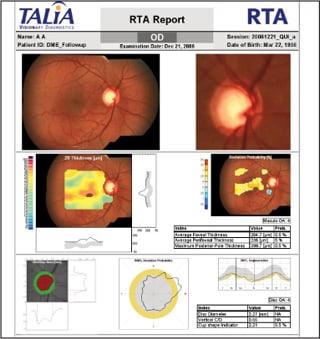
Figure 2. Referral to a retina specialist for consideration of laser treatment should be made for this diabetes patient due to the retinal thickening within 500μm of the foveal center.
Dr. Gerson says that a comanaging optometrist must maintain a solid understanding of not only these but all current standards of retinal care. He also notes that an increasing number of retina specialists are now using anti-VEGF agents off-label to treat patients with diabetic retinopathy. Therefore, it's important to discuss with comanaging partners how that might change the timing of referrals.
Diagnostic Equipment
Optometrists also should have knowledge of the diagnostic equipment used in retinal care. Dilated fundus exams are central to screening patients for signs of retinal pathology and monitoring after retinal procedures, but specialized equipment can expand the optometrist's role in comanagment. A fundus camera, for example, is helpful for monitoring changes over time. “Often, no specialized equipment is needed, but what instruments you do or don't have should be discussed with the specialists with whom you plan to work,” Dr. Warren says. As part of his clinical exam protocol, Dr. Warren uses the Talia Retinal Thickness Analyzer (RTA 5) for screening and for comparing the status of the macula from visit to visit.
Dr. Gerson uses the Optos P200 Optomap (an ultra-widefield imaging device) and the Optovue RTVue (a Fourier domain OCT machine) for monitoring changes over time. “You don't need these instruments to follow patients' retinal health, but they provide additional information for ruling out or confirming pathology and guiding referrals,” he says. OCT is especially useful in his practice for detecting recurring leakage in AMD patients who've undergone anti-VEGF treatments and for quantifying macular edema in diabetes patients.
Dr. Way uses OCT in his practice as well as an Optomap ultra-widefield imaging device, which serves as a screening tool and a means of gathering more detailed information about the health of the peripheral retina.
A Clear Path for Progress
Along with considering acquiring additional equipment, optometrists should apply for inclusion on medical insurance panels. “If patients can't use their insurance to access your care, they may be inclined to go elsewhere,” Dr. Way says.
With that final piece in place, putting your education and experience to work for your patients shouldn't be a problem. From Dr. Brownlow's point of view, most surgeons have moved past the criticisms that had been leveled against comanagement in the past and are working with optometrists on post-op care. Furthermore, he says, “There are no legal or governmental challenges to comanagement, provided all decisions are made with each patient's best interests in mind.” Regarding retinal coman-agement in particular, Dr. Way believes surgeons are becoming more aware of the in-depth education optometrists receive and are therefore increasingly comfortable working with them. nOD
REFERENCES
- Diabetic Retinopathy Study Research Group. Photocoagulation treatment of proliferative diabetic retinopathy: The second report of diabetic retinopathy findings. Ophthalmology. 1978;85:82–106.
- Diabetic Retinopathy Study Research Group. Photocoagulation treatment of proliferative diabetic retinopathy. Clinical application of Diabetic Retinopathy Study (DRS) findings. DRS Report Number 8. Ophthalmology. 1981;88:583–600.
- Diabetic Retinopathy Study Research Group. Indications for photocoagulation treatment of diabetic retinopathy: DRS Report Number 14. Int Ophthalmol Clin. 1987;27:239–253.
- Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report Number 1. Arch Ophthalmol. 1985;103:1796–1806.
- Early Treatment Diabetic Research Study Research Group. Treatment techniques and clinical guidelines for photocoagulation of diabetic macular edema. Early Treatment Diabetic Retinopathy Study Report Number 2. Ophthalmology. 1987;94:761–774.
- Early Treatment Diabetic Retinopathy Research Group. Photocoagulation for diabetic macular edema: Early Treatment Diabetic Retinopathy Study Report Number 4. Int Ophthalmol Clin. 1987;27:265–272.
- Early Treatment Diabetic Retinopathy Research Group. Early photocoagulation for diabetic retinopathy. Early Treatment Diabetic Retinopathy Study Report Number 9. Ophthalmology. 1991;98:766–785.
- Early Treatment Diabetic Retinopathy Research Group. Fundus photographic risk factors for progression of diabetic retinopathy. Early Treatment Diabetic Retinopathy Study Report Number 12. Ophthalmology. 1991;98:823–833.
- Early Treatment Diabetic Retinopathy Research Group. Focal photocoagulation treatment of diabetic macular edema. Relationship of treatment effect to fluorescein angiographic and other retinal characteristics at baseline. Early Treatment Diabetic Retinopathy Study Report Number 19. Arch Ophthalmol. 1995;113:1144–1155.
- Diabetic Retinopathy Vitrectomy Study Research Group. Early vitrectomy for severe vitreous hemorrhage in diabetic retinopathy. Two-year results of a randomized trial. Diabetic Retinopathy Vitrectomy Study Report 2. Arch Ophthalmol. 1985;103:1644–1652.
- Diabetic Retinopathy Vitrectomy Study Research Group. Early vitrectomy for severe proliferative diabetic retinopathy in eyes with useful vision. Clinical application of results of a randomized trial. Diabetic Retinopathy Vitrectomy Study Report 4. Ophthalmology. 1988;95:1321–1334.