


Leading the Way in Anterior Segment and Glaucoma Evaluation
From injury to advanced disease, SD-OCT has changed the way we see structure and pathology.

By Joseph Sowka, OD, FAAO, Diplomate
At my university, we upgraded to spectral domain optical coherence tomography (SD-OCT) to enhance diagnosis and tracking and increase efficiency. Today's SD-OCT devices are accurate, effective and easy to use.
The change from Stratus time domain OCT to Cirrus HD-OCT has given us significant advantages. The resolution went from 10 microns down to 5 microns, which creates a much higher quality image. Time domain gave us “wow-factor” views of the histological cross-section, but today's SD-OCT devices offer far more detail, so our ability to view structures and pathology is phenomenal.
In clinical practice today, SD-OCT has a 3-part role: anterior segment evaluation, glaucoma diagnosis and tracking and retinal applications. In this article, I will review some of the anterior segment and glaucoma applications of Cirrus HD-OCT to show how I am utilizing the benefits of this technology.
Anterior Segment Examination
Using Cirrus HD-OCT to examine the anterior segment, we gain several diagnostic advantages, most notably in measuring the angle, seeing the status of the iris, identifying anatomic landmarks and visualizing the cornea.
• Angle of the anterior chamber: Gonioscopy is an important tool in glaucoma management, but it is intimidating to some practitioners. One reason is that it can be hard to judge anatomy correctly and is not easily used to calculate a gonioscopic angle. Another reason is that there exists a false perception that it creates significant discomfort to the patient (which it does not). Anterior Segment imaging on Cirrus, on the other hand, provides us with an excellent cross-section of the anterior chamber angle. It helps to confirm gonioscopic findings and show the anterior chamber angle in a way that gonioscopy cannot. However, at this time, OCT does not replace gonioscopy in the diagnosis and management of glaucoma, but it does serve as a valuable adjunct.
Rather than looking directly into the angle, we can view it clearly in profile and measure it easily. I have patients with some form of angle closure or at risk of angle closure. Those with angles that are 15° or less on OCT are at risk for closure.
• Iris status: Using SD-OCT, we can examine the status of the iris and receive detailed answers to some very important questions: What is happening anatomically? Is the iris flat, convex or concave? Is the angle of incidence occludable or non-occludable (Figure 1)?
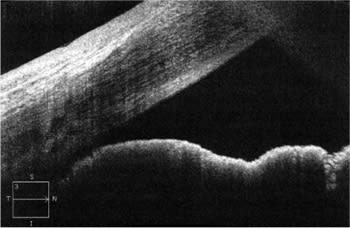
Figure 1. Large last roll of iris and occludable angle in plateau iris syndrome.
SD-OCT also provides insight about issues that arise when patients undergo laser iridotomy or other anterior segment procedures.
• Anatomic landmarks in the anterior chamber: With all of the imaging techniques we use, we are looking for high image quaility, which will allow us to see certain anatomic landmarks. This can be very challenging with older modalities, but SD-OCT's high level of detail makes these landmarks much clearer. Now we're able to capture landmarks, such as Schlemm's canal, Schwalbe's line, the trabecular meshwork and the ciliary face.
In concert with gonioscopy, which is still a necessary test, SD-OCT provides a clearer picture of what is happening in the anterior chamber.
• Cornea: SD-OCT has many capabilites when it comes to the cornea. Using this technology, we can see the epithelium, the tear layer, Bowman's membrane and even the endothelium. We can evaluate the homogenous clarity of the stroma. We can even measure corneal thickness virtually anywhere on the cornea (Figure 2).
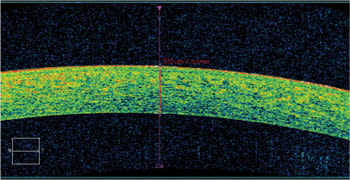
Figure 2. A caliper allows for thickness measurement of the cornea.
In addition, we can use SD-OCT to look at corneal pathologies. It's an excellent imaging device for keratoconus, scarring, edema and other problems that affect the cornea.
The total picture of the anterior segment that SD-OCT affords — angle, iris, anatomic landmarks and cornea — has been a strong motivator for me to use the technology more often in practice and to encourage colleagues to do so.
Diagnosing Glaucoma
We diagnose glaucoma by collecting and interpreting data in a number of ways, then subjecting data to our experienced eyes and clinical judgment. There are three parts to the process of SD-OCT interpretation in my practice.
1) I review the Cirrus printout, which provides accurate measurements and compares the patient's measured retinal nerve fiber layer (RNFL) against normative data to help determine how each patients' RNFL may differ from healthy eyes.
2) Based on clinical experience looking at many SD images in patients with all stages of glaucoma, I place a value judgment. Am I more accustomed to seeing these findings in a normal population or an abnormal population? Is the RNFL normal or abnormal? This is the subjective interpretation of the SD OCT printout.
3) Finally, I determine how this data fits into the clinical picture. Does the patient have risk factors for glaucoma? Is there a suspicious nerve? Is there anything else that corroborates glaucoma? An abnormal RNFL by SD-OCT in the absence of any other clinical features or risk factors for glaucoma is not reason enough for me to make a diagnosis or begin treatment.
All three of these steps make up the glaucoma diagnosis. No high-tech device will make a glaucoma diagnosis or tell you with 100% certainty if a patient's eye is normal or abnormal. That's why we're here. As clinicians, we have to review all of the information together to make the proper diagnosis. That said, SD-OCT is a valuable adjunct because it makes diagnosis easier and helps us feel more confident in our decisions.
Using Cirrus HD-OCT in Glaucoma Patients
Glaucoma diagnosis is one of the most common uses for SD-OCT and a big motivator for many practitioners to acquire this technology. SD-OCT provides images that are much clearer than those provided with time domain OCT, thus enabling us to more easily diagnose or rule out glaucoma
With Cirrus HD-OCT, we can look at the RNFL, measure it and analyze the results. The software also helps us to do one of the most important and, until recently, difficult tasks of glaucoma detection: combine structural and functional measurements.
The first glaucomatous change can be structural (disc or RNFL) or functional (visual field loss). SD-OCT helps us diagnose and manage glaucoma by giving us an assessment of anatomic structure which can be combined with the function assessment provided by visual fields to increase diagnostic accuracy. We use the technology not only to diagnose glaucoma, but also to monitor and manage the disease in both straightforward and complex cases.
OCT and functional assessment is used in conjunction with applanation tonometry and gonioscopy in diagnosing and managing patients with glaucoma. After all, glaucoma is a clinical diagnosis we make not on the basis of one parameter, but on the basis of several. We have to look at everything (Figure 3).
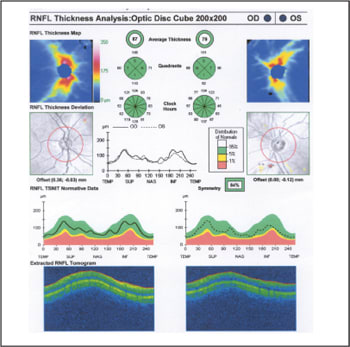
Figure 3. A patient with elevated intraocular pressure from pigment dispersion syndrome demonstrates a normal RNFL OU.
Because Cirrus provides a great deal of data for us, I like to use a number of features on the analysis when I am evaluating a glaucoma suspect. First, I look at the RNFL Thickness Map, where bright reds and yellows (warm colors) in an hourglass pattern reflect that the RNFL is anatomically thick. When the thick areas begin to diminish, I am concerned the patient has had some loss of RNFL.
I check the Deviation Maps, which compare the patient's measured data against a normative database to show how they differ. This is very important to me because it helps me identify clinically significant abnormalities in the RNFL. While the Deviation Maps from the Cirrus can show areas where measurements are statistically significant, it is up to the clinician to determine whether or not the results are clinically significant.
I also look at the temporal-superior-nasal-inferior-temporal (TSNIT) analysis, which compares the patient's measured data to a normative database. Where patient results depart from normal, I have to look more carefully at the disc in those areas and check for corresponding visual field deficits (Figure 4).

Figure 4. A normal RNFL OD and abnormal RNFL OS in a patient with unilateral glaucoma.
All of these data and interpretations help me get a clear picture of what is going on anatomically in my patients' eyes. SD-OCT gives me more information than I had in the past. Normative data comparisons and new, pristine images enhance my ability to detect glaucoma and anterior segment problems and decide on a treatment. SD-OCT helps me put all of the important pieces together.
Dr. Sowka is a Professor at Nova Southeastern University College of Optometry, where he serves as Chief of the Advanced Care Center and Director of the Glaucoma Service. He is a Diplomate of the American Academy of Optometry's Disease Section, Glaucoma Subsection.
Editor's note: As of March 2010, optic nerve head analysis is available on Cirrus HD-OCT. It uses the same data that is captured for RNFL analysis, and provides automated identification of the optic disc and cup boundaries and measures the neuroretinal rim with excellent reproducibility.