


diabetes
Managing The Diabetic Patient
Your role as a member of this patient's healthcare team is comprised of two crucial parts.
Blair B. Lonsberry, O.D., M.S., M.Ed, F.A.A.O., Portland, Ore.
A 56 year-old white male “walk-in” patient presents to the office because he broke his glasses. He travels a lot as a truck driver and, as a result, hasn't had his eyes examined in several years. The patient reports no current medical conditions or taking any medications.
His best-corrected visual acuity is 20/20 OU. Evaluation of the fundus reveals dot hemorrhages and microaneurysms OU. I ask the patient: “Have you ever been tested for diabetes?” He replies: “No.” I then explain to him that I'm noticing changes in his retinae that indicate he may have diabetes. I ask him about recent weight changes, increased thirst and urination — other symptoms of the disease, which he denies experiencing. Next, I strongly recommend he see his primary care physician for a diabetes work-up. I hand him my card and tell him to have his doctor call me once he secures an appointment. The patient tells me he doesn't have a regular doctor due to his traveling.
Several hours later, I receive a call from an emergency room physician. (Because the patient doesn't have a regular primary-care doctor, he chose to report to an emergency room for an assessment.) The physician informs me that the 56 year-old patient is there and asked that she call me. I tell her about the changes to the patient's retinae, and that these changes are indicative of diabetic retinopathy. I then explain that due to these findings, I'm concerned the patient's blood sugar levels are significantly high and have likely been so for a prolonged period of time.

PHOTO CREDIT: DIANA L. SHECHTMAN, O.D., F.A.A.O.
This patient displayed mild to moderate non-proliferative diabetic retinopathy.
Several days later, I receive a call from the patient. He says his blood sugar reading that day was 405, and his A1c was 10.1. He thanks me and says he never would've known he'd had diabetes — at least not for some time — had I not caught it.
If you haven't had a similar patient encounter, you likely will. O.D.s are often the first members of the healthcare team to discover diabetes via the presence of the disease's ocular manifestations. Also, an estimated 24 million people (approximately 8% of the population) in the United States alone have diabetes. And, approximately 3.3 million members of this group report visual impairment, and a large proportion due to the ocular manifestations of their diabetes.1
Given these facts, it's imperative we, as, O.D.s, know our role as a member of the diabetic patient's healthcare team. This role is comprised of two crucial parts:
Educator
When diabetic patients present for their eye exams and report they're under the care of a primary care physician or endocrinologist, never assume the patient has been thoroughly educated regarding the disease and its related management.
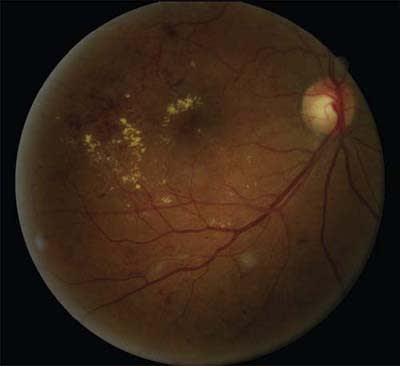
PHOTO CREDIT: DIANA L. SHECHTMAN, O.D., F.A.A.O.
This patient showed severe non-proliferative diabetic retinopathy with clinically significant macular edema.
In fact, a recent study showed that almost a third of patients given the diabetes diagnosis recalled leaving their primary care physician's office with minimal or no plan for action (e.g. a clear treatment plan, support, education and follow-up.)2 This same study revealed that what patients are told about diabetes at the time of diagnosis and the recommendations that are made immediately after are linked to how patients feel about their disease and how well they will manage their disease later.
Therefore, when these patients are in your exam chair, set aside time to educate them on the importance of annual comprehensive dilated eye exams (e.g. the potentially devastating and permanent vision changes that can result from untreated retinal complications), good blood glucose level, blood pressure, cholesterol control and the necessity of a good diet and exercise. This education should also include the importance of compliance with your instructions/recommendations in minimizing the potential affects the disease can have on the eye (e.g. diabetic retinopathy, cataract and glaucoma).
Diabetic retinopathy, as illustrated in the case of the 56-year-old man, is a frequent complication of both Type 1 and 2 diabetes, which is among the top five most common causes of legal blindness in the United States.3 A total of 95% of Type 1 and 60% of Type 2 patients will demonstrate some signs of diabetic retinopathy 20 years post-diagnosis.3 (See “Depression and Diabetes,” below.)
The Diabetes Control and Complications Trial revealed that blood glucose level control can slow both the advent and progression of diabetic retinopathy. Also, the Action to Control Cardiovascular Risk in Diabetes (ACCORD) Eye study, revealed that intensive blood sugar control compared with standard-blood sugar control reduced diabetic retinopathy progression by roughly one-third, from 10.4% to 7.3% through four years. In addition, this practice has been shown to decrease the need for scatter laser treatment.3
The problem: Many diabetic patients often present not knowing their last blood glucose level, or they comment that their primary care physician checks their A1c levels every three months and tells them whether they're “good or not.” Although A1c levels indicate a patient's blood glucose levels through a three-month time period, they do not provide real-time information regarding the daily fluctuations in blood glucose levels that occur with changes in diet and physical activity levels. And, because they're collected every three months, it, therefore, takes three months to assess the effectiveness of patient lifestyle modifications.
A randomized clinical-based interventional study on the management of new-onset Type 2 diabetes patients revealed that when patients monitored their own blood glucose levels on a daily basis, they were empowered to achieve nutritional and physical activity goals.4
Because early intervention is so important in preventing vision loss, as part of our role as educator we should encourage our diabetic patients to monitor their own blood glucose levels on a daily basis and to keep a diary on these levels. We should then send a written report to the patient's primary care physician outlining the eye exam's results along with the patient's latest glucose level and reported range. This step helps our patients, and shows/reinforces to the primary care doctor the importance of our role as a member of the patient's healthcare team.
| Depression and Diabetes |
|---|
| Several studies reveal that patients who have diabetes are twice as likely to have co-occurring major depression as non-diabetic patients, and 11% to 15% of patients who have diabetes meet the criteria for a major depressive disorder.13,14 It's also interesting to note that a history of major depression raises the risk twofold for the development of Type 2 diabetes.13 Depression has been linked to poor compliance in patients. For patients who have diabetes, this non-compliance can reveal itself in medication regimens, failure to refill medications or decreased adherence to exercise and diet recommendations. Obviously, patients who aren't taking their medications or following diet/exercise recommendations run the risk of major organ failure and blindness. Evidence suggests, however, that patients who undergo appropriate treatment for their depressive symptoms can improve and maintain their blood glycemic control and decrease the likelihood of developing diabetic complications.14 Keep in mind that depression and diabetes have many overlapping symptoms, including energy loss, weight gain or loss, appetite change, mood swings, etc. This makes the depression diagnosis challenging. Therefore, as part of your overall assessment of the patient, be sure to include a mini-mental exam to determine whether the patient has depression. This includes assessing the patient's orientation (e.g. whether he's aware of the time and place), his general mood, appearance (e.g. is the patient well groomed or wearing clothing inappropriate for their age or weather) and asking questions, such as “how are you?” etc. Additionally, you may want to have the patient take a depression test, which includes questions, such as “Do you feel sad, unhappy, hopeless, or otherwise “down in the dumps”?” Also, remember that family history, having multiple medical problems (particularly chronic conditions, such as pain) predispose patients to depression, and therefore, should be noted in the patient's medical record. |
Clinician
Diabetic retinopathy is likely the most well known complication associated with diabetes, and it's potentially the most visually devastating. Clinically significant macular edema (CSME) and proliferative diabetic retinopathy (PDR) development are the major concerns for our patients. Because CSME and PDR may develop sans symptoms, we, as clinicians, must carefully evaluate the fundus for any changes. Ocular coherence tomography (OCT) and/or fluorescein angiography may be indicated to confirm the diagnosis. OCT, unlike fluorescein angiography, is non-invasive, and has, therefore, become a mainstay technology for the diagnosis and management of diabetic retinopathy.
Should we identify CSME, the patient should be referred to a retinal specialist for focal/grid laser treatment, kenalog or anti-vascular endothelial growth factor (VEGF) injections.5 Recent studies reveal that the combination of focal laser treatment with an anti-VEGF medication is likely the most beneficial for the treatment of macular edema. Specifically, the use of anti-VEGF has the potential to rapidly reduce the macular edema and improve vision fast, while a focal/grid laser results in a likely long-term stabilization of vision (potentially reducing the number of anti-VEGF injections required to minimize the macular edema).6
Should our evaluation reveal PDR, we should refer the patient to a retinal specialist for panretinal photocoagulation (PRP), with or without the additional use of anti-VEGF medication. Remember: Anti-VEGF medication use is “off-label,” so we must develop a close relationship with the retinal specialist with whom we're comanaging to find out their typical/usual treatment protocol for patients who have CSME or proliferative changes. We, as the comanaging clinician, want to be able to counsel the patient as to what, exactly, he can expect when he presents to the retinal specialist.
If the patient receives treatment, such as PRP for PDR, he is at an increased risk of developing post-operative complications, such as macula edema (thickening) and tractional retinal detachment.7 (Depending on your relationship with the retinal specialist, you may be responsible for monitoring the patient for post-operative complications.)
Several studies have demonstrated a four-fold increase in cataracts in diabetic patients younger than age 65 and a twofold excess in prevalence in diabetic patients older than age 65.8 Although the pathogenesis of diabetic cataract development is not fully understood, researchers believe it's related to the role of the polyol pathway (conversion of glucose to sorbitol via the enzyme aldose reductase).8 Intracellular accumulation of sorbitol leads to osmotic changes, which then results in the collapse and liquefaction of lens fibers. This altered osmotic stress results in cataract development more frequently and at an early age in diabetic patients.
The overall outcomes of cataract surgery are excellent in patients who have diabetes. However, these patients may have poorer visual outcomes than patients who don't have diabetes. This is because the surgery may cause a rapid acceleration of retinopathy, and cystoid macular edema (CME) is more prevalent in these patients. The worst outcomes are typically seen in operated eyes that have active PDR and/or pre-existing CSME.8
CME also has an increased prevalence in diabetic patients post-cataract surgery.9 As a result, many cataract/retinal surgeons choose to pre-treat diabetes patients with a topical non-steroidal anti-inflammatory (NSAID) drug t.i.d. to q.i.d. upwards of two weeks prior to the surgery and throughout the postop period. Studies suggest that NSAIDs may reduce the incidence, duration and severity of CME by inhibiting the release of prostaglandins and the subsequent breakdown of the blood-retina barrier 9,10 The NSAID prescription is within our jurisdiction as the comanaging eyecare practitioner.
Something else to keep in mind: Because diabetic patients have been known to have an increased prevalence of ocular surface disease, such as ocular dryness, this will affect the patient's visual outcome post-surgery, particularly in patients receiving premium intraocular lenses. As a result, we, as the co-managing clinician, must aggressively manage any ocular surface disease pre- and post-operatively to ensure patient comfort and success.10
In addition, we, as clinicians, play a role in the regular post-operative care of these patients by prescribing steroid/antibiotic drops, closely monitoring healing and being alert for any complications, such as posterior capsule opacification.
An association between glaucoma and diabetes continues to be debated . Several studies have demonstrated that patients who have diabetes have a higher prevalence of glaucoma (5%) vs. patients without diabetes (2%).11 Other studies, have not supported these findings, which makes this a tenuous association. However, diabetes does affect the small blood vessels, resulting in poor perfusion. Glaucoma is ultimately a decrease in perfusion to the optic nerve, resulting in damage. Additionally, patients who have diabetes have impaired auto-regulation of blood flow, which may affect a patient's regulation of blood flow to the optic nerve.12
We should educate patients who have diabetes about a possible increased risk of glaucoma and the importance of regular eye exams. Also, we should work up these patients for glaucoma. Should glaucomatous findings, such as increased cup-to-disc ratio, elevated/borderline intraocular pressure (IOP) or visual field defects appear, we should aggressively treat the patient to establish a low target IOP.
Because that 56-year-old truck driver was just passing through, I never saw him again. That said, I'm confident he's now undergoing treatment/management for diabetes and that, as a result, his long-term risk of cardiovascular and ocular complications has been significantly reduced. The reason for my confidence: As educator/clinician, I prompted him to seek a diabetes work-up the very same day he saw me. By adapting these two roles, you'll likely have the same effect on your patients. OM
1. Centers for Disease Control and Prevention. Diabetes Public Health Resource. 2007 National Diabetes Fact Sheet. www.cdc.gov/diabetes/pubs/pdf/ndfs_2007.pdf. Accessed November 12, 2010.)
2. Polonsky, WH, Fisher L, Guzman S, et al. Are patients’ initial experiences at the diagnosis of Type 2 diabetes associated with attitudes and self-management over time? Diabetes Educ. 2010 Sep-Oct;36(5):828-34.
3. The Diabetes Control and Complications Trial Research Group. Lifetime benefits and costs of intensive therapy as practiced in the Diabetes Control and Complications Trial. JAMA. 1996 Nov 6;276(17):1409-15.
4. Duran, A, Martin P, Runkle I, et al. Benefits of self-monitoring blood glucose in the management of new-onset Type 2 diabetes mellitus: The St. Carlos Study, a prospective randomized clinic-based interventional study with parallel groups. J Diabetes. 2010 Sep;2(3):203-11.
5. The Read-2 Study Group. Primary End Point (Six Months) Results of the Ranibizumab for Edema of the macula in
Diabetes (READ-2) Study. Ophthalmology 2009 Nov;116(11):2175-81.
6. The Diabetic Retinopathy Clinical Research Network. Randomized trial evaluating ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology. 2010 Jun;117(6):1064-1077.
7. Gündüz K, Bakri SJ. Management of proliferative diabetic retinopathy. Compr Ophthalmol Update. 2007 Sep-Oct;8(5):245-56.
8. Pollreisz, A, Schmidt-Erfurth U. Diabetic cataract-pathogenesis, epidemiology and treatment. J Ophthalmol. 2010:608751
9. O'Brien TP. Emerging guidelines for use of NSAID therapy to optimize cataract surgery patient care. Curr Med Res Opin. 2005 Jul;21(7):1131-7.
10. Shah AS, Chen SH. Cataract surgery and diabetes. Curr Opin Ophthalmol, 2010 Jan;21(1):4-9.
11. Bernth-Petersen, P and Bach E. Epidemiologic aspects of cataract surgery: III: Frequency of diabetes and glaucoma in a cataract population. Acta Ophthalmol (Copenh). 1983 Jun;61(3):406-16.
12. Jeganathan VS, Wang JJ, Wong TY. Ocular associations of diabetes other than diabetic retinopathy. Diabetes Care. 2008 Sep;31(9):1905-12.
13. Osborn CY, Kozak C, Wagner J. Theory in practice: helping providers address depression in diabetes care. J Contin Educ Health Prof. 2010 Summer;30 (3):172-9.
14. Noel LT. An ethical/racial comparison of causal beliefs and treatment preferences for the symptoms of depression among patients with diabetes. Diabetes Educ. 2010 Sep-Oct;36(5):816-27.

| Dr. Lonsberry is a professor of optometry at the Pacific University College of Optometry in Portland. Also, he's clinic director of the Portland Vision Center and has spoken about the care of the diabetic patient at optometric trade shows. E-mail him at blonsberry@pacificu.edu, or send comments to optometricmanagement@gmail.com. |