


macular degeneration
Kicking the “A” Out of AMD
Research suggests the disease process may start earlier in life than first thought and that nutritional supplementation at an earlier age may be beneficial for at-risk patients.
JOHN WARREN, O.D., Racine, Wisc.
According to the National Eye Institute of the National Institutes of Health, the greatest risk factor for age-related macular degeneration is age. Because signs of macular degeneration typically do not manifest until after age 50, physicians have traditionally referred to the disease as “senile” or “age-related.” Because exposure to ultraviolet and high-energy blue light and oxidative stress occur throughout life, it would make sense that the disease process for macular degeneration may begin as early as the third decade of life, long before it manifests as drusen and retinal pigment epithelium changes.
For this reason, I believe it's time to kick the “A” out of AMD and prevent, identify and treat the disease as what it really is: the sum of years of oxidative and photo stress damage. In this article, I explain how macular pigmentary changes can predict AMD and the steps we can take to counteract these changes.
Nutritional supplementation
Traditionally, Western medicine has been a reactive science, but in the last decade, it has started to shift more toward preventative or proactive care. The use of statins for early treatment of coronary artery disease is one example. In my opinion, there is no reason such a model should not be applied to macular degeneration. Undoubtedly, many patients will develop macular degeneration, regardless of the preventative steps, but there is simply too much sound data to provide only reactive care of macular degeneration.
The ARED Study, for example, found that taking a specific high-dose formulation of antioxidants and zinc significantly reduces the risk of advanced AMD and its associated vision loss.1 Investigators found the benefits of supplementation with the AREDS formulation could result in as much as a 25% reduction in the development of macular degeneration. These benefits could not be gained by dietary nutritional intake, so supplementation was required. The AREDS did not include any of the more recently recommended carotenoids, such as lutein, zeaxanthin and meso-zeaxanthin. Recent research by investigators has shown substantial links between the presence of these pigments in the macula and the risk of developing macular degeneration.2,3
As shown in Figure 1, as levels of lutein, zeaxanthin and meso-zeaxanthin rise, the incidence of macular degeneration decreases. The risk for a patient in the lower groups is double that for a patient who had pigment density in the average range. The corollary is that patients with average levels of lutein, zeaxanthin and meso-zeaxanthin have half the risk of developing AMD as those with low levels of these pigments.
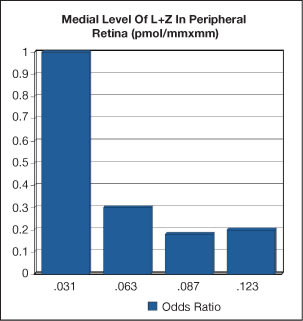
Figure 1. As levels of lutein, zeaxanthin and meso-zeaxanthin rise, the incidence of AMD decreases.
Research has also shown that ingesting lutein, zeaxanthin and meso-zeaxanthin results in an increase in the density of macular pigmentation. It then follows that ingesting these pigments will reduce a patient's risk of developing macular degeneration.
Approximately 5% of the population will not deposit lutein and zeaxanthin in the macula, so it is important to measure the effect of nutritional supplementation on macular pigment density.
The MPPD factor
As with coronary artery disease, the sooner we identify at-risk patients and institute preventative measures, the more likely they are to reduce their risk. By recognizing that macular degeneration is not a disease of advanced age, but a disease of damage over time, we have a chance to reduce the risk of vision loss.
Now that we understand the importance of identifying patients who have low levels of lutein, zeaxanthin and meso-zeaxanthin, our next step is to learn how to determine a patient's macular protective pigment density (MPPD) and put these findings into clinical practice. Heterochromatic flicker photometry (HFP) is a scientifically validated method of measuring macular pigment density. Thus, it is the ideal instrument to identify patients who are at risk of developing macular degeneration and to measure the effect of nutritional supplementation in these patients. The MacuScope (U.S. distribution by Marco Ophthalmic, Inc., Jacksonville, Fla.) and the QuantifEYE (ZeaVision, LLC, Chesterfield, Mo.) perform these functions.
MPPD testing in practice
We perform MPPD testing during pretesting, after we take the patient's history and measure visual acuity, but before corneal topography to prevent any visual disturbance by the topography rings.
I discuss the MPPD findings with patients during their examination, usually while reviewing the family and social history in my EMR. This allows me to tie the biggest risk factors (or hopefully lack thereof) together. If a patient has low MPPD or other significant risk factors, I start the conversation about supplementation, but I withhold final recommendations until after I perform the internal examination.
For patients who have normal to high levels of MPPD, I usually recommend a broad-spectrum nutritional supplement, mostly because I practice in the upper Midwest where the typical diet is not high in fresh, green vegetables, especially in the winter months. I find that many, if not most, of my patients over the age of 50 are already taking some form of supplement.
For patients who have low MPPD levels, I first discuss typical risk reduction activities. The first steps I discuss are smoking cessation and reduction of fat in the diet because these factors are linked to macular degeneration and also to lower MPPD levels. About 90% of my patients are wearing ophthalmic lenses that absorb UV radiation or contact lenses with sunglasses, so I don't spend much time talking about UV protection, but I do mention it.
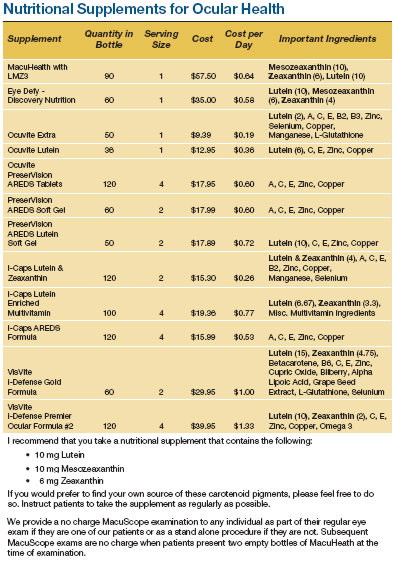
The next step is to review a patient's current nutritional supplementation. I specifically ask about lutein, zeaxanthin and meso-zeaxanthin intake. Many patients are already taking a supplement that contains some lutein, but typically not enough, and either a small amount or no zeaxanthin or meso-zeaxanthin. I briefly review information about the absorption and synthesis of nutrients, as well as their antioxidant and photoprotective roles in macular health. I then tell patients that they cannot improve their MPPD appreciably without direct ingestion of zeaxanthin and meso-zeaxanthin. The chart below shows the ingredients and concentrations of many of the available supplements (courtesy of Wes Kemp, O.D.).
Patients who start supplementation receive a 6-month supply (180 tablets) and are scheduled for a follow up MPPD examination in 6 months where I expect to see a modest rise in their MPPD levels. I provide this brief encounter at no cost to patients who are actively supplementing.
If patients choose to not follow my recommendation for supplementation, I simply document their decision and let them know that we will retest their MPPD at their next examination and revisit the topic as necessary.
My patients have responded well to this approach, regardless of whether we identify a potential problem and take action or if we determine that they are at no increased risk for macular degeneration compared to the general population.
Whether or not to charge patients for MPPD testing is an individual decision. Some practices will choose to measure MPPD in all patients who fit the criteria (age, family history, past ophthalmic history, etc.) and include the testing in their examination fee. This has the benefit of removing any financial barrier to testing your patients. It is what I have chosen to do, with an increase of $5 in my examination fee when we added the MPPD test to our clinical testing protocols. We run HFP testing on all patients over the age of 30.
Some practices charge patients a separate fee when measuring MPPD. This has the benefit of creating a value for the testing, but some patients who would benefit from MPPD testing and intervention will opt out because of the extra cost. This choice should not be taken lightly, nor should it be a snap judgment. Talking to your patients about the importance of MPPD testing will help you gauge their interest and determine how to position the testing in your practice.
Proactive choice
Using heterochromatic flicker photometry, we can measure MPPD and identify patients who have a higher risk of developing macular degeneration later in life. This instrument also enables us to measure the impact of treatment on the macular pigment density, so that we can confidently recommend scientifically directed supplementation to patients who have the most to gain from it. OM
- Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol. 2001;119:1417-1436.
- Bone RA, Landrum JT, Mayne ST, Gomez CM, Tibor SE, Twaroska EE. Macular pigment in donor eyes with and without AMD: a case-control study. Invest Ophthalmol Vis Sci. 2001;42:235-240.
- Beatty S, Murray IJ, Henson DB, Carden D, Koh HH Boulton ME. Macular pigment and risk for age-related macular degeneration in subjects from a northern European population. Invest Ophthalmol Vis Sci. 2001;42:439-446.

|
Dr. Warren is in private practice in Racine, Wisc. He also provides onsite nursing home care 1 day per week in the Milwaukee area. Dr. Warren has no financial interest in the sale of any products mentioned in this article. Dr. Warren can be reached at: jwarrenod@gmail.com. |