


retina
RISING TO THE AMD Challenge
A thorough, systematic approach to managing patients will help preserve vision.
JAY M. HAYNIE, O.D., F.A.A.O., Tacoma, Wash.
More than 10 million people in the United States have decreased vision resulting from age-related macular degeneration (AMD), making it the country's leading cause of legal blindness.1,2 Additionally, 200,000 new cases of choroidal neovascularization (CNV) are diagnosed each year, and those numbers are expected to climb as the population ages.3 These predicted increases will test our ability to provide optimal care to our patients who have or are at risk for AMD.
A frustration we face when managing AMD is that patients often are diagnosed too late for us to institute risk-reduction measures and preventative therapy. For example, based on the findings of the Age-related Eye Disease Study (AREDS), we know that people who are at high risk of developing advanced AMD can reduce their risk by as much as 25% by adding antioxidants and zinc to their diets.4 Our ability to help these patients can be hampered by a lack of patient education and the limitations of current self-monitoring methods.
In this article, I discuss the protocols we follow at Retina & Macula Specialists to educate our patients and to manage their risk factors and disease.
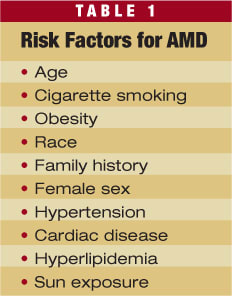
Education and self-monitoring
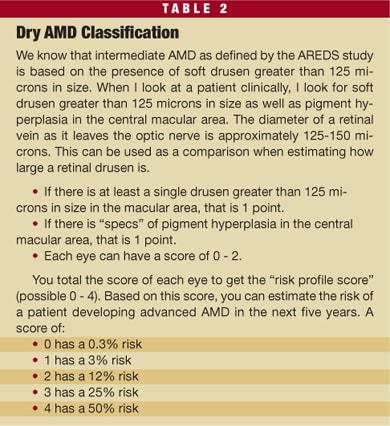
To provide our patients with the best care possible, we must thoroughly educate them about their condition and its associated risk factors. When my patients present with AMD, I walk them through the 10 most common risk factors (see Table 1) and develop their personal risk profile. Based on this profile, I suggest lifestyle modifications, which may include smoking cessation, cholesterol reduction, weight reduction and instruction on smart nutritional choices. I also classify each patient's risk of conversion from dry AMD to wet AMD on a scale of 0 to 4 based on the presence and size of drusen and the presence of pigment hyperplasia. I then interpret the score to determine our course of action, including, how often we see the patient, how often we test the patient for conversion and the time frame for behavior modification. (See “Dry AMD Classification,” Table 2, below.)
Monitoring patients for conversion from dry to wet AMD is just as important as patient education to ensure timely and successful treatment. Currently, the only subjective test available for self-monitoring is the Amsler grid. Unfortunately, the Amsler grid is not effective in detecting subtle signs of disease progression. In fact, studies show it has a sensitivity of only 29%.5 Often, by the time the Amsler grid begins to look distorted, the patient's condition has progressed significantly.6
Although I still recommend that patients use the Amsler grid, I also encourage them to incorporate self-monitoring into their daily activities, using objects they see every day to test their vision. Observing something that is already part of their normal viewing habits makes it easier for them to be compliant. I also recommend monocular viewing. Patients can check for changes in their vision by simply covering one eye and then the other while engaging in normal activities, such as watching TV or reading. If they notice a difference in vision between their eyes, they know to come into the office as soon as possible.
In addition to educating patients about self-monitoring, we use in-office protocols to identify CNV. In our practice, this means monitoring with preferential hyperacuity perimetry (Foresee PHP, Reichert Ophthalmic Instruments, Depew, N.Y.) and confirmation with optical coherence tomography (OCT) and intravenous fluorescein angiography (IVFA) by our retina specialist.
Create a safety net
In my opinion, PHP technology is one of the more valuable additions to our offices. It is a simple test that takes less than 5 minutes per eye and allows us to detect CNV at its earliest stages. The PHP offers 82% sensitivity and 88% specificity, which means it will provide consistently reliable results. By testing quarterly with PHP technology, we create a “safety net” for our patients because it can differentiate between intermediate dry AMD and wet AMD, allowing us to confirm CNV and start treatment before visual changes take place.7
Through the development of treatments for wet AMD, we have learned that a patient's visual outcome is directly related to the size of his lesion. The larger the lesion, the worse the prognosis. A CNV membrane can grow about 20 microns per day or about 600 microns in a month. If a patient is seen only twice a year, he/she could develop a new lesion immediately after an examination, and then present to his next appointment with a lesion as large as 3,600 microns. At this point, up to 5 lines of vision may have been lost. This is why we monitor our high-risk patients quarterly using PHP. Even if a patient's disease converts to wet AMD the next day, the lesion will grow to only 1800 microns between tests. At the patient's next examination, the PHP will identify an abnormality, and we will still be able to implement treatment before his functional vision deteriorates.
Case study
A 74-year-old woman presented to our office with a history of vision loss in her right eye for 7 years resulting from wet AMD. She was referred by her local optometrist with a 3-week history of decreased vision in her left eye with metamorphopsia. Her vision was CF OD and 20/50+2 OS; IOP measured 16 mm Hg OD and 14 mm Hg OS with normal anterior segment findings.
The patient's ocular history included AMD in both eyes and cataracts. The patient was a smoker and had a history of hypertension, elevated cholesterol, congestive heart failure, prior heart attack and depression. She used medications for her known medical conditions, as well as nutritional supplements of fish oil and lutein for her ocular conditions.
Preferential hyperacuity perimetry showed an abnormality (Figure 1), and conversion to CNV was confirmed by OCT (Figure 2) and IVFA (Figure 3). Fundus photography (Figure 4) showed an area of hemorrhage nasal to the fovea, but no obvious subretinal fluid or subretinal exudate. Using PHP, we were able to rule out vision impairment due to cataracts and our retina specialist started treatment for wet AMD. After treatment with bevacizumab (Avastin, Genentech), triamcinolone acetonide and bevacizumab again, each one month apart, the patient's metamorphopsia in the left eye resolved. If her CNV had gone undetected any longer, it is likely she would not have had such a successful outcome.
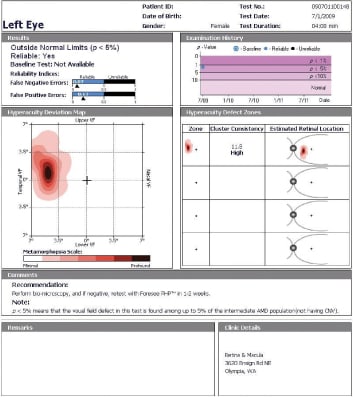
Figure 1. PHP test results reveals a dense scotoma of the left eye.
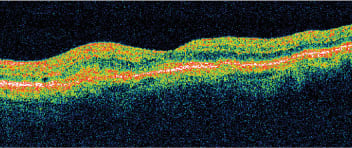
Figure 2. OCT shows an area of elevation localized to the retinal pigment epithelium.
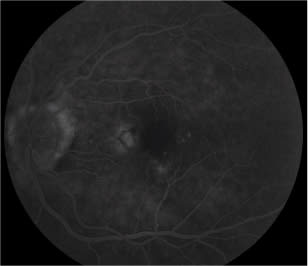
Figure 3. Fluorescein angiography identifies a classic choroidal neovascularization that corresponds precisely to the scotoma identified with PHP.
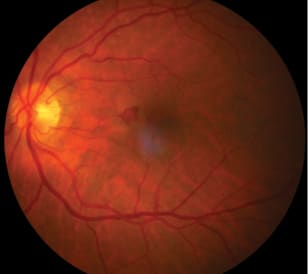
Figure 4. Fundus photography shows an area of hemorrhage nasal to the fovea. No obvious subretinal fluid or subretinal exudate is seen, however.
A lifetime of healthy vision
Although we face many challenges when managing AMD, it is imperative to meet those challenges head on. Our patients may not be as compliant as we'd like, or they may be referred too late for us to use our full armamentarium. If we as optometric physicians are to be on the forefront of disease management, however, we owe it to our patients to provide the best care possible through education, monitoring and testing devices, and advice on nutritional supplements. As AMD continues to affect more of our patients, we must strive to give them exactly what they deserve, which is a lifetime of healthy vision. OM
1. Singerman LJ, Miller DG. Pharmacological treatments for AMD. Rev Ophthalmol. 2003;10:88-94.
2. Vision Problems in the U.S., Prevent Blindness America: www.preventblindness.org/vpus.
3. Friedman DS, O'Colmain BJ, Munoz B, et al. Prevalence of age-related macular degeneration in the United Sates. Arch Ophthalmol. 2004;122:564-572.
4. Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol. 2001;119:1417-1436.
5. Zaidi FH, Cheong-Leen R, Gair EJ, et al. The Amsler chart is of doubtful value in retina screening for early laser therapy of subretinal membranes. The West London Survey. Eye. 2004; 18:503-508.
6. Fine AM, Elman MJ, Ebert JE, Prestia PA, Starr JS, Fine SL. Earliest symptoms caused by neovascular membranes in the macula. Arch Ophthalmol. 1986;104:513-514.
7. Loewenstein A, Malach R, Goldstein M, et al. Replacing the Amsler grid: a new method for monitoring patients with age-related macular degeneration. Ophthalmology. 2003:110:966-970.

|
Dr. Haynie is the executive clinical director for Retina & Macula Specialists, with offices in Olympia, Renton and Tacoma, Wash. He writes and lectures on retinal disease, new management strategies, updates on current diagnostic instrumentation and its role in management of ocular disease. He has no financial interest in PHP technology. |