


optic nerve
More Than Just a Number
When taking a second look at the optic nerve, look to the traditional measurements … and beyond.
Austin Lifferth, O.D., F.A.A.O.
Lousiville, Ken.
Over the years, our understanding of glaucoma has matured. More specifically, the definition has advanced from an eye disease that was focused on an eye pressure greater than 21mmHg to a more refined and sophisticated description that describes glaucoma more as a multifactorial “ … chronic, progressive disease that most often presents with characteristic optic nerve damage, nerve fiber layer defects and subsequent visual field loss.”1 Several studies have reinforced this definition and emphasized the importance of a thorough, systematic, stereoscopic optic nerve evaluation. This is because these “characteristic optic nerve damage [and] nerve fiber layer defects” can precede the onset of visual field loss by more than five years in 50% to 80% of our patients.2 Therefore, these findings reinforce the responsibility that we, as eyecare practitioners, have to carefully evaluate the optic nerve for any early evidence of glaucomatous damage and prevent potential functional visual field loss.
No ideal numbers
Notably missing from this more evolved definition, and for a very good reason, is a pre-determined cup-to-disc ratio that would conveniently and quickly classify one nerve as normal and another nerve as glaucomatous. This ideal number does not exist because more than an occasional overlap of the normal optic nerve cup-to-disc ratio number with the glaucomatous optic nerve cup-to-disc ratio number exists � and vice versa. To further clarify, one study concluded that not only was there a surprising spectrum between normal and glaucomatous eyes but that also a cup-to-disc ratio of up to 0.9 can be considered normal depending on the optic nerve size, a variable not accounted for solely with quantitative evaluation.3 In other words, the cup-to-disc ratio number alone cannot tell us whether a nerve is healthy or pathologic for disease.
However, and rather ironically, we still use a number to provide us with a description of the optic nerve based on Armaly's Structural Systems from the 1960s.4 Although primarily quantitative in its description, this valuable method remains the standard worldwide for both diagnosing glaucomatous damage and monitoring for glaucomatous progression in the both clinical and research settings. This method has remained relevant because it's easy to learn, to teach and to apply than many other contemporary methods for staging glaucomatous optic nerve disease.5 Although easy and enduring, this method for evaluating glaucoma has certain inherent limitations that are often overlooked when we take our “first look” at the optic nerve. To better demonstrate these limitations and to reinforce the need to develop and utilize methods that are more qualitatively descriptive, the images to the right are presented.
The first look
Without any additional supportive information, testing or the benefit of stereopsis, which image(s) suggest glaucomatous optic nerve damage?
At first glance, and in the context of the cup-to-disc ratio staging system, one would justifiably be more concerned about glaucoma in Figures A and C due to the larger cup-to-disc ratio appearance relative to Figure B. This rapid assumption is due to an unintentional and unspoken subtle bias that suggests that the larger the cup-to-disc ratio, the greater the likelihood of glaucomatous optic nerve damage. Although this conjecture is commonly correct, it is not clinically conclusive.
The second look
Is there more to evaluating the optic nerve than just recording a cup-to-disc ratio? Is it more than just a number?
For instance (and without stereopsis), in Figure A, can you appreciate the average-to-large optic nerve size and relatively healthy neuroretinal rim appearance that conforms to the helpful inferior, superior, nasal, temporal (I.S.N.T.) rule?
Did you notice the inferior rim thinning evident in Figure B despite the relatively small cup-to-disc ratio?
How about the relatively small nerve with inferior rim thinning, associated early betazone peripapillary atrophy and Drance retinal hemorrhage observed in Figure C?
Interestingly, we can see that if all other factors were equal, two different patients with a cup-to-disc ratio of .75 each (Figure A and C) could potentially have two different diagnoses and, therefore, two different prognoses and treatments. In other words, a quantitative evaluation provides just a number and potentially an incorrect diagnosis with likely over- or under-treatment.
These images and this discussion describes the possible status quo in regard to glaucomatous optic nerve evaluation. Without caution, we can commonly slip into a relaxing, casual quantitative evaluation of the optic nerve and just put down a number. From these images, it is obvious that a second look provides a more qualitative evaluation that is more comprehensive and more specific than the standard quantitative evaluation. In other words, the qualitative evaluation allows us to treat the patient with better quality and with better congruency with our current understanding and definition of glaucoma. Indeed, as with many other aspects of glaucoma care, optic nerve evaluation for glaucoma is more than just a number.
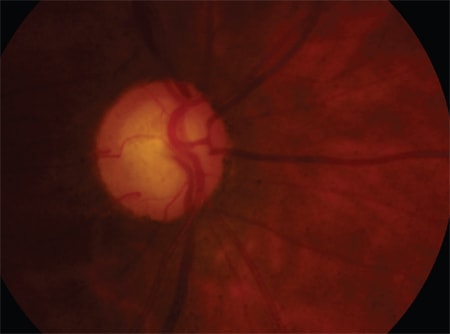
Figure A: C/D ratio ~.75
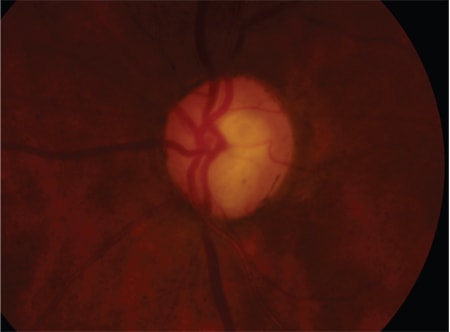
Figure B: C/D ratio ~.65
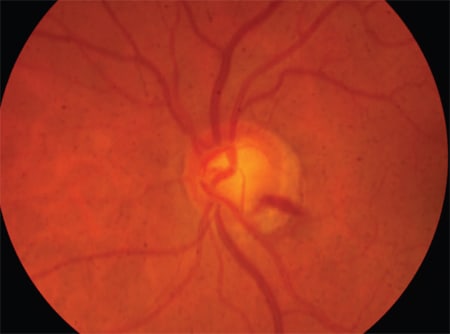
Figure C: C/D ratio ~.75
More than just a number …
So what staging systems or methods are available to better qualitatively evaluate the optic nerve head for glaucoma?
The Focusing Ophthalmology on Reframing Glaucoma Evaluation (F.O.R.G.E.) 5-rule (R) Method and the Spaeth Disc Damage Likelihood Scale (DDLS) Systemare two resources that not only compliment the standard Armaly method but also have a synergistic diagnostic benefit for both the doctor and the patient.5-7 For purposes of review, these methods are briefly described below.
The 5-Rs, or rules, of F.O.R.G.E., include:
► evaluation of optic disc size
► neuroretinal rim size and shape
► evaluation of retinal nerve fiber layer
► presence of parapapillary atrophy
► presence of retinal or optic disc hemorrhages.
The best way to understand this method is to take a second look at Figure C. Before assigning it a cup-to-disc ratio number, examine carefully the scleral ring size to determine the size of the optic nerve. This is best accomplished by direct stereoscopic examination with your preferred fundus lens, with its associated magnification adjustment and the illumination beam height. This first step is so important because it has been shown that glaucoma is often under-diagnosed in small nerves and overdiagnosed in large nerves.5
Next, examine the rim size, contour and color in relation to the optic nerve size looking for notching associated with early glaucomatous visual field damage or pallor that extends beyond the cup-to-disc ratio suggestive of other types of optic neuropathies. This is also a good time to apply the I.S.N.T. Rule, which suggests that in more than 60% of the population, the inferior rim is successively broader than the superior, nasal, and temporal rim, respectively, in normal-shaped eyes and is independent of the optic nerve size.8
As you extend outward in all directions from the rim, carefully evaluate the retinal nerve fiber layer quality looking for splinter or wedge defects (which are best seen with red-free illumination) and increased peripapillary vessel clarity that results from the associated nerve fiber loss observed best with normal illumination.
Look closely in the peripapillary region for atrophy that is commonly seen with these structural changes. Particularly, when two zones of peripapillary atrophy are present, the inner circumference beta-zone peripapillary atrophy (with its characteristic increased choroid vessel and scleral clarity), is more specific for glaucomatous optic nerve damage than the more common and less alarming outer circumference hypopigmented alphazone peripapillary atrophy.
Finally, with further inspection, look carefully for the often transient feathery retinal/disc hemorrhages suggestive of poor control and common in patients who have normal tension glaucoma. By applying the 5-R, Figure C becomes more than just a number and, after a second look, helps establish a qualitative baseline optic nerve evaluation.
A scale for disc damage
The DDLS system allows the observer to qualitatively describe the optic nerve's rim-to-disc ratio at its narrowest point.7 Or, if no rim tissue actually remains, the circumferential extent of this rim absence is measured in degrees.
By focusing on the rim-todisc ratio, rather than the cup-to-disc ratio, the examiner is more aware of the 5-R's, as shown above, and can better predict the amount of correlating visual field damage that commonly develops approximately halfway through this staging system. Even more, these stages follow a natural course history characteristic of glaucomatous optic nerve damage and provide a much needed and heavier emphasis on moderate-to-end-stage glaucomatous cupping.
By examining the rim and trying to carefully note how much rim is left over, this system is a repeatable way to carefully discern how much functional rim remains, not how much is gone. This remaining rim is then highly correlated with the amount of visual field remaining and an indicator of the patient's functional vision capabilities. If we are to treat patients and not just numbers (e.g. intraocular pressures, cup-to-disc ratios, etc.), this is a highly qualitative and highly reproducible staging system that ensures better quality patient care.
Worth a second look
In addition to the standard quantitative cup-to-disc ratio staging system and as we consider the above systems, I invite you to take a second look. Look for the 5-Rs individually, and then combine them collectively with a rim-to-disc ratio analysis to increase your diagnostic power. As you look for and utilize these qualitative methods in close complimentary connection with the traditional quantitative cup-to-disc ratio evaluation, you'll be better able to see the optic nerve for how it really is and quickly realize that it is more than just a number. OM
1. Optometric Clinical Practice Guideline: Care of the Patient with Open Angle Glaucoma. www.aoa.org/documents/CPG-9.pdf. (Accessed July 2011.)
2. Quigley HA, Katz J, Derick RJ, et al. An evaluation of optic disc and nerve fiber layer examinations in monitoring progression of early glaucoma damage. Ophthalmology. 1992 Jan;99(1):19-28.
3. Jonas JB, Gusek GC, Maumann GO. Optic disc, cup and neuroretinal rim size, configuration and correlations in the normal eyes. Invest Ophthalmol Vis Sci. 1988 Jul;29(7):1151-8.
4. Armaly MF. The optic cup in the normal eye. I. Cup width, depth, vessel displacement, ocular tension and outflow facility. Am J Ophthalmol. 1969 Sep; 68(3):401-7.
5. Susanna R., Vessani RM:. New findings in the evaluation of the optic disc in glaucoma diagnosis. Curr Opin Ophthalmol. 2007 Mar;18(2):122-8. Review.
6. Fingeret, M, Medeiros FA, Susanna R, et al. Five rules to evaluate the optic disc and retinal nerve fiber layer for glaucoma. Optometry. 2005 Nov;76(11): 661-8.
7. Spaeth, GL, Lopes JF, Junk AK, et al. Systems for staging the amount of optic nerve damage in glaucoma: a critical review and new material. Surv Ophthalmol. 2006 Jul-Aug;51(4):293-315.
8. Budde WM, Jonas JB, Martus P, Gr�ndler AE. Influence of optic disc size on neuroretinal rim shape in healthy eyes. J Glaucoma. 2000 Oct;9(5):357-62.

|
Dr. Lifferth practices at Bennett & Bloom Eye Centers. He completed internships specializing in ocular disease at the VA Hospitals in Huntington, W.V. and Lexington, Ken., as well as an extensive residency at the Veterans Affairs Medical Center in Huntington. E-mail him at austinlifferth@yahoo.com, or send comments to optmoetricmanagement@gmail.com. |