


contact lens
Myopia Control
Understand why and how you should offer overnight corneal reshaping.
Michael J. Lipson, O.D., F.A.A.O., Livonia, Mich.
“Every six months we need to get my child stronger glasses. Why are my child's eyes changing so fast?” What do you say to the parents of this child when this question is posed to you? About 30% of the U.S. population is myopic, so this is a question you are likely to hear every day in your practice. Prescribing the updated spectacle prescription is an option, but have you considered overnight corneal reshaping (OCR)?
Here, I describe why you should consider offering this procedure, how to become OCR certified, the ideal candidates, how you can successfully dispense these lenses and how to effectively manage these patients to decrease the likelihood of adverse events.
Why OCR?
There are six reasons you should consider offering OCR to myopic children:
(1) It has been shown to slow and sometimes arrest myopia progression. Studies on myopic progression in both the U.S. and around the world have revealed that efforts to slow myopic progression with pharmaceutical agents (pirenzepine, atropine), spectacle undercorrection, spectacle bifocals and spectacle progressive lenses have had little or no effect on slowing the rate of myopic progression.1-5 Studies on the efficacy of OCR, however, have shown that these FDA-approved RGP lenses can significantly reduce the rate of myopic progression. In addition, other studies have revealed OCR can result in the complete arrest of myopic progression in children. In both study types, myopia progression was evaluated by comparing pre-treatment refraction and axial length to post-treatment findings.6-9 The reason for these outcomes: The change in central corneal curvature and overall corneal asphericity also changes the peripheral refraction that reduces or eliminates hyperopic defocus.10,11 The high majority of OCR patients I've worked with have shown stable refractions through many years and have not required changes in lens parameters to maintain stable findings for topography, unaided visual acuity and axial length. In fact, in a four-and-a-half year retrospective study I did representing 507 patient years of OCR, 90% of these patients attained 20/25 acuity or better.12 The purpose of the study was to compare the efficacy and safety of OCR in children younger than age 12 to those older than age 12.

Dr. Lipson with a new OCR patient and his mother as the nine-year-old patient prepares to apply his OCR lens.
(2) It has been shown as safe in children. One study revealed that three-fifths of 23 OCR subjects, ages eight to 11, had mild corneal staining in the morning, and one third had mild staining in the afternoon, though none experienced lasting adverse visual effects during the study period.6 The study sought to describe the refractive error, visual changes and slit lamp observations associated with OCR in children through a six-month period. The researchers examined the subjects within one hour of waking and six hours later at one day, one week, two weeks, one month, three months and six months post the first night of OCR. The researchers assessed visual acuity, manifest refraction, slit lamp exam findings and corneal topography at each visit.
Another study, which included 16 subjects, ages 10 to 16, revealed that the short-term correction (e.g. six months) of mild-to-moderate myopia with OCR was safe in children and adolescents.13 These patients were fit empirically with OCR lenses and were evaluated at one day, one week, one month, two months, three months and six months. An average of 40% of eyes revealed some type of corneal staining between the one-week and six-month visits, but no serious adverse events were reported.
In the OCR outcomes study I did, three minor adverse events (corneal abrasions) occurred, but none resulted in a loss of best-corrected visual acuity, and all patients returned to OCR and continue to wear OCR lenses.
(3) They can improve a child's quality of life. Research has shown that spectacle-wearing children vs. non-spectacle wearing children are more likely to be the victims of physical or verbal bullying.14 In addition, research has revealed that myopic children report better vision-related quality of life with contact lenses vs. glasses.15 When patients see clearly upon removal of their correction—a majority of my patients have reported unaided vision better than the vision they had with glasses—they've said the lenses made participating in activities, such as sports, much more enjoyable.
(4) Parents appreciate their purpose and convenience. Most of the parents with whom I've discussed these lenses have said that if OCR can slow myopic progression, they'd like to give that advantage to their children. In addition, they've told me they appreciate that the lenses are at less of a risk for loss or damage, as they don't leave the house.
(5) They create patient loyalty. Offering OCR in my practice has enabled me to create patient loyalty in that patients appreciate the uniqueness of a service that they can't get from many eyecare providers. This patient loyalty has led to several referrals, making OCR a huge practice builder.
(6) They increase practice revenue. Because OCR is a unique service, fees are based on our professional service and expertise. Fees for a “normal” case across the country range from $900 to $2,000 with higher fees for “complex” cases, such as high myopia (>−4.50D), high astigmatism (>1.25D) or unusual topography (high or low eccentricity or decentered apex). These fees, in combination with patient loyalty and retention, can create a very profitable situation for a new practitioner coming into a practice as well as for the established practitioner who wants to add “something new” to the practice. Insurance carriers generally have a fixed reimbursement amount for contact lenses. So, another financial point to consider is that the majority of OCR fees are not covered by insurance. Therefore, it's a source of insurance-independent, non-discounted income.
Becoming certified
To become OCR certified, first contact one of the manufacturers for information, education and certification tests. (See “FDA-Approved Overnight Corneal Reshaping Lenses,” below.) Second, attend fitting seminars and practice management sessions on the subject. Third, seek fitting workshops and lectures at contact lens meetings. Finally, find a mentor who has worked with OCR lenses, and stay in close contact during your first few cases. Finding a mentor could be through the various lens manufacturers (calling their customer service department), an organization, such as the Orthokeratology Academy of America (http://ok global.org) or the Gas Permeable Lens Institute (www.rgpli.org).
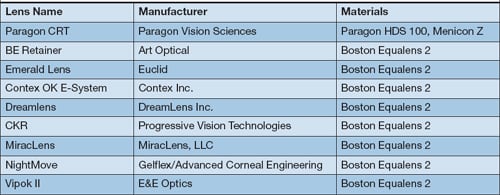
FDA-Approved Overnight Corneal Reshaping Lenses
Patient candidacy
Ideal OCR candidates include: (1) patients whose myopia is between −.75D and −4.50D and whose astigmatism is less than 1.25D, (2) patients with normal corneal topography and (3) patients who are strongly motivated to be free of glasses during their waking hours. Motivation is the most difficult to gauge. Ask the child, not the parent: “How do feel about wearing contact lenses?” or “How do you feel about wearing glasses?” Their reaction to these questions will help assess the child's interest in using contact lenses. Occasionally, we find parents are more motivated than the child. Remember: The child wears the lenses each night. To maintain best vision and eye health, compliance with wearing time and lens care procedures is imperative for long-term success.
How to offer OCR
I've found that presenting OCR as one of the vision correction options available for my patients has been a successful means of educating patients about these lenses. For example, at the conclusion of an exam on a 12-year old myope, I address both the child and his parents in the following way: “Evan, you are nearsighted and need vision correction to see properly for many of your daily activities like school and sports. We have a few different ways to accomplish that, which include: glasses worn during the day, contact lenses worn during the day or contact lenses you wear only when sleeping.” At this point, more often than not, the patient and/or his parent say: “Wow. I've never heard about lenses that are worn only at night. How do they work?” From there, I provide the patient and his parent with printed materials, videos and my enthusiastic, trained staff to answer the additional multitude of questions that usually follow, and educate the patient and his parent on both the benefits and risks of OCR.
Although the initial cost of OCR may be higher than traditional contact lenses or glasses, presenting the costs of each modality through the course of four- to five-years makes the cost of OCR much more comparable. In our office, the initial fee covers diagnostic fitting, lenses and all follow-up visits for the first six months. Thereafter, annual exams are done at the standard fee of an established patient for a comprehensive exam. Six-month check-ups are done as an office visit that is about 60% of the annual exam. If patients have “vision” insurance, it usually covers the annual exams but not the six-month follow-up.
Effective management
As is the case with traditional contact lenses, OCR is not without its risks. These include infectious keratitis, corneal abrasion, irregular corneal astigmatism and corneal ulcers.16-18 That said, I've had success in decreasing the likelihood of adverse events by doing the following:
► Getting the right fit. In our office, we've found that corneal topography, corneal diameter (HVID) as well as manual keratometry measures are needed for the best starting point. Although various OCR lens designs exist, there are characteristics common to all of them. Specifically, the posterior surface of the lens contains a number of different curves that are of reverse geometry design, in which the secondary curves are steeper (more curved) than the central curve. Also, they are made of high dK materials approved for overnight wear. Achieving good centration is the key to success in providing ideal vision correction. Ideal centration creates a treatment zone centered over the visual axis to maximize visual acuity and minimize glare. Experience with a particular brand will make you more comfortable in making changes that perfect the fit. But, as with all contact lenses, one design doesn't work perfectly on every patient.
► Providing patient education. My staff instructs both the patient and his parent on how to apply, remove and care for the lenses. They also discuss the importance of following the prescribed wearing schedule and practicing personal hygiene (washing hands prior to insertion and removal, etc.) to minimize the chance of complications, such as corneal abrasions, infection and corneal ulcer. Serious complications, though rare, are linked to non-compliance, such as not using proper solutions, inadequate lens cleaning and case contamination.16,19 I personally review and reinforce proper lens care at every follow-up visit.
► Scheduling several follow-up appointments. In my practice, we schedule the patient for the following day after sleeping with the lenses for the first night. At this appointment, we test unaided visual acuity, assess corneal topography (to evaluate lens position during sleep) and perform a slit lamp evaluation to assess corneal health. Follow-up visits are routinely scheduled after the first night of wear, one week, one month, three months and six months. At all follow-up visits, lenses are changed as necessary to optimize lens centration, corneal health and unaided visual acuity. In addition, I encourage patients to present if they experience blurred vision, discomfort with or without lenses or consistent redness. Finally, I re-emphasize the importance of complying with the specific directions given to them regarding lens wear and care. Thereafter, I see OCR patients every six months.
In OCR, success depends on equal parts of practitioner expertise, proper follow-up care, lens maintenance and cleaning and good doctor-patient communication. I highly recommend using a fitting agreement/informed consent to detail risk/benefit, follow-up care, fees, office policies, emergency contact information and expectations.
Because OCR can be a safe, effective and profitable vision correction option, you should consider offering it. So, the next time a parent asks you, “Is there anything you can do to stop or slow the vision changes we are seeing in my child?”, now you have something encouraging and exciting to talk about. OM
1. Tan DT, Lam DS, Chua WH, et al. One-year multicenter, double-masked, placebo-controlled, parallel safety and efficacy study of 2% pirenzepine ophthalmic gel in children with myopia. Ophthalmology 2005 Jan; 112(1):84–91
2. Lee JJ, Fang PC, Yang IH, et al. Prevention of myopia progression with 0.05% atropine solution. J Ocul Pharmacol. Ther. 2006 Feb;22(1):41-46
3. Fulk G, et al. Seasonal variation in myopia progression and ocular elongation. Optom Vis Sci. 2002 Jan;79(1):46-51
4. Goss DA, Rainey BB. Relation of childhood myopia progression rates to time of year. J Am Optom Assoc. 1998 Apr;69(4):262-6.
5. Gwiazda J, Hyman L, Hussein M, et al. A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Invest Ophthalmol Vis Sci. 2003 Apr;44(4):1492–500.
6. Walline JJ, Rah MJ, Jones LA. The Children's Overnight Orthokeratology Investigation (COOKI) pilot study. Optom Vis Sci 2004 Jun; 81(6):407–413.
7. Cho P. Ocular Changes and Myopia Progression After 12 months Orthokeratology Lens Wear. Presented at the 9th International Conference on Myopia, Hong Kong and Guangzhou, China, November 10–14th, 2002.
8. Cho P, Cheung SW, Edwards M. The longitudinal orthokeratology research in children (LORIC) in Hong Kong: a pilot study on refractive changes and myopic control. Curr Eye Res 2005 Jan;30(1):71-80.
9. Walline JJ, Jones LA, Sinnott LT. Corneal reshaping and myopia progression. Br J Ophthal 2009 Sep;93(9):1181-5.
10. Smith EL, et al. Peripheral vision can influence eye growth and refractive development in infant monkeys. Invest Ophthal Vis Sci. 2005 Nov;46(11):3965-3672.
11. Smith EL 3rd, Hung LF, Huang J. Relative peripheral hyperopic defocus alters central refractive development in infant monkeys. Vis Res 2009 Sep;49 (19):2386-2392.
12. Lipson MJ. Long-term clinical outcomes for overnight corneal reshaping in children and adults. Eye Cont Lens 2008 Mar;34(2):94-99.
13. Mika R, Morgan B, Cron M, Lotoczky J, Pole J. Safety and efficacy of overnight orthokeratology in myopic children. Optometry. 2007 May;78 (5):225-31.
14. Horwood J, Waylen A, Herrick D, et al. Common visual defects and peer victimization in children. Invest Ophthal Vis Sci. 2005 Apr;46 (4):1177-81.
15. Rah M, Walline JJ, Jones-Jordan LA, Sinott LT, et al. Vision specific quality of life of pediatric contact lens wearers. Optom Vis Sci. 2010 Aug;87(8):560-6.
16. Van Meter WS, Musch DC, Jacos DS, et al. Safety of overnight orthokeratology for myopia: a report by the American Academy of Ophthalmology. Ophthalmology. 2008 Dec;115(12):2301-2313.
17. Hiraoko T, Matsumoto Y, Okamoto F, et al. Corneal higher-order aberrations induced by overnight orthokeratology. Am J Ophthalmol. 2005 Mar;139(3):429-36.
18. Hiraoko T, Furuya A, Matsumoto Y, et al. Quantitative evaluation of regular and irregular corneal astigmatism in patients having overnight orthokeratology. J Cataract Refract Surg. 2004 Jul;30(7):1425-9.
19. Saviola JF. The Current FDA view on overnight orthokeratology: how we got here and where we are going. Cornea 2005 Oct;24(7):770-1.

| Dr. Lipson is an assistant professor at the University of Michigan's Kellogg Eye Center. He specializes in contact lenses and sports vision. E-mail him at mjlipson@umich.edu, or send comments to optometricmanagement@gmail.com. |