


meibomian gland dysfunction
MGD: Get Your Ducts in a Row
Meibomian gland dysfunction may comprise the majority of dry eye disease. Here's how you can correctly diagnose and treat it.
Jerry R. Paugh, O.D., Ph.D., F.A.A.O., Fullerton, Calif.
Anecdotal evidence in our clinic suggests a prevalence rate for meibomian gland dysfunction (MGD) (both hypo-, and hypersecretory—see below) of approximately 75% of all dry eyes evaluated. In addition, the recent International Workshop on Meibomian Gland Dysfunction (MGD) reports, sponsored by the Tear Film & Ocular Surface Society (www.tearfilm.org) and published in a special issue of Investigative Ophthalmology & Visual Science (IOVS), suggest a population prevalence of MGD in persons older than age 40 ranging from 3.5% to 60%, depending on study diagnostic criteria.1 (See insert: “Meibomian gland dysfunction: What is it, why does it occur and how may it be treated?”) In fact, the MGD Workshop reports reveal that the condition may actually comprise the majority of dry eye disease. Given MGD's prevalence and the devastating effect its symptoms (ocular dryness, itching and/or photophobia) can have on one's quality of life, it's essential, we as eyecare practitioners, correctly diagnose and treat it. This article explains how to arrive at the MGD diagnosis and the current treatment options available.
Distinguishing signs
The Definition and Classification Subcommittee of the MGD Workshop defines the condition as “a chronic, diffuse abnormality of the meibomian glands commonly characterized by terminal duct obstruction and/or qualitative/quantitative changes in glandular secretion.”2 Related conditions are blepharitis (both anterior and posterior). Although MGD may progress to an inflammatory state, it can also remain inflammation free in its early stages. The two types of MGD are hyposecretory and hypersecretory.2
To ensure the correct diagnosis and management of MGD, you must distinguish aqueous tear deficiency (ATD) dry eye disease (e.g., Sjögren's syndrome and non-Sjögren's syndrome) from MGD (hyposecretory and hypersecretory). The following tests can be used clinically to differentiate ATD from MGD:
► Meibomian gland expression (must be done prior to meiboscopy). A cut-point > Grade 1 on a 0 to 3 scale (3 = tooth-paste) reveals MGD as long as the tests for aqueous tear sufficiency (i.e., the Schirmer test [see below] and/or tear meniscus height) are normal.
► Transillumination meiboscopy for gland dropout/atrophy. A cut-point > Grade 1 or ~ 25% of glands missing reveals MGD. (See figure 1.)
► Schirmer test without anesthetic. In our clinic, we use the Schirmer test without anesthetic for five minutes. The reason: If a patient cannot produce aqueous tears under irritating conditions, he probably is not producing enough aqueous tears. A cut point of < 5mm suggests ATD.
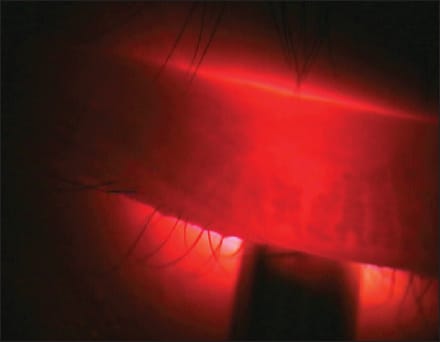
FIGURE 1: Transillumination biomicroscopy demonstrating gland dropout. Normal glands are dark, absorbing light. The central two glands appear one-half atrophied, while there are longer, but still partially atrophied glands on either side of the transilluminator tip. The relative white space between acini is termed “glandular distention,” which is an indication of partial gland atrophy.
The required evidence
In contradistinction, if symptoms and signs of dry eye exist, yet the tear volume and production appear normal, evidence of meibomian gland compromise is required to make a definitive diagnosis of MGD. A diagnostic trend that appears to be gaining momentum in this realm is the summation of several eyelid margin and meibomian gland ordinal scales to develop a total meibomian gland rating scale.3,4 The meibomian-gland specific work-up on which these scales are based:
► Eyelid margin evaluation. Perform biomicroscopy using a moderately “white” illumination and 10X to 16X magnification. While general dry eye signs are noted (e.g., tear debris, obvious epithelial disruptions, etc.), the goal is to observe and rate as present (1) or absent (0) four specific marginal signs: (1) orifice metaplasia (the presence of white shafts extending above the orifice); (2) vascularity of the palpebral conjunctiva (vessel engorgement—also called “brush-marks”); (3) plugged or capped orifices (perhaps with a membranous cap); (4) and lid margin irregularity (notching often seen as the eyelid tissue contracts).5 Each sign is rated as “0” or “1” if absent or present for a total score of 0 to 4.
While many clinical scales use integer intervals to form an ordinal scale of increasing severity, in our clinic, we use at least 0.5 scale unit increments for ordinal scales (e.g. grade 1.5 corneal staining) or even 0.1 unit increments for research purposes. The reason: A compelling study revealed using finer increments allows for improved discrimination among patients and enhanced monitoring of progress from one visit to another.6 (While using finer increments at first may seem challenging, through time it becomes second nature.)
► Meibomian gland expression: The four current approaches to gland expression: digital pressure, the use of a cotton swab, the Mastrota paddle and a meibomian gland expression device developed by optometrists Donald Korb and Caroline Blackie. To employ digital pressure, gently, yet firmly, press one finger against the lower eyelid, applanating the lid margin against the globe. Hold for three-to-seven seconds for the secretion to express. To use the cotton swab, approach the eyelid tangentially (i.e., flat side toward the margin), and take care to prevent lid eversion. (See figure 2, below.) Next, instruct the patient to look up (to avoid brushing the cornea and to allay apprehension) and blink normally. Now, press gently and hold for three-to-seven seconds (it often takes time for the meibum to express, and when it first appears, it often looks like a small volcano eruption). To employ the Mastrota paddle, slip the device behind the lower eyelid and apply either digital pressure or cotton swab pressure to the outer eyelid for three-to-seven seconds to manually express the glands (considered forceful expression with backing). To use the meibomian gland expression device, press it against the eyelid margin and depress until its plunger retracts slightly. The device is held in place three-to-seven seconds and the secretion graded.7 The grading system for secretion is: Grade 0 = normal, clear, may have a few particles; Grade 1 = opaque with normal viscosity; Grade 2 = opaque with increased viscosity; and Grade 3 = severe thickening (toothpaste). Be sure to grade the entire lower eyelid, and estimate the average secretion grade.

FIGURE 2: Illustration of Q-tip method of meibomian gland expression technique. The Q-tip is pressed tangentially and gently against the eyelid margin and the margin observed through the biomicroscope. After three-to-seven seconds, the secretion should manifest as a pool or small “eruption.”
► Gland dropout/atrophy via meiboscopy. Use transillumination biomicroscopy. Specifically, have the patient seated comfortably in the biomicroscope, looking up and blinking normally. Next, use 16X magnification. The transilluminator everts the eyelid to expose the glands in the tarsal plate. (See figure 3, below.) Beginning at the temporal extent of the lower eyelid, count the number of half- and whole-missing glands. (Find a complete gland as a reference in a given eyelid.) We assume 24 glands are present in a normal eyelid and calculate a percentage of gland dropout.8 For example, six total glands missing of 24 possible represents 25% dropout, or approximately a Grade 1 dropout, depending on the criterion (different percentages of dropout exist for various grades). In our clinic, we've found success by grading gland dropout as follows:3 Grade 0.0 = no dropout; Grade 1.0 = 25.0%; Grade 2.0 = 50.0%; Grade 3.0 = 75.0% and Grade 4.0 = 100%. (Transillumination biomicroscopy requires some practice, though I've found it can usually be mastered after using it on five to 10 patients.)

FIGURE 3: The transilluminator everts the eyelid to expose the glands in the tarsal plate.
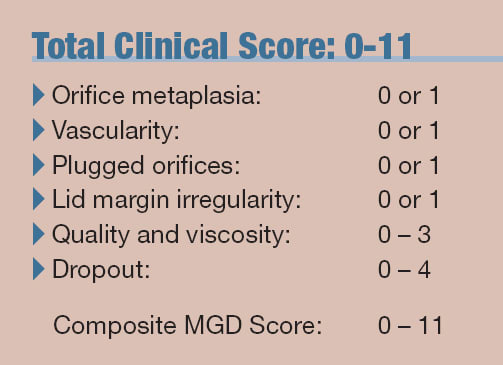
This summed approach to MGD diagnosis, using several tests, provides a numerical score with the MGD diagnosis at a score of three or greater, so long as secretion and dropout scores are > Grade 1, and there is at least one positive eyelid sign. (See “Total Clinical Score,” below.) Further research needs to be undertaken to determine precise scale cut-points relative to test sensitivity, specificity and Receiver Operating Characteristic curves.
Current treatments
The goal of MGD management is to two-fold: (1) to assist the remaining meibomian glands in producing more and better quality lipids to restore ocular surface homeostasis and (2) reduce inflammation of the glands, which is nearly always present. In our clinic, we've found that the best course of action in achieving these goals is to follow this stepladder of treatment (keep in mind that each of these therapies can be used solely or in combination, relative to the individual patient's condition):
► Warm compresses and eyelid massage, b.i.d. (once in the morning and once at night). The warmth helps to overcome the elevated melting point of lipids inspissated within the glands. Similarly, the massage helps to express the oils, so that the glands become unblocked. Eyelid massage also brings blood flow to the eyelid area containing the glands, which can help remove inflammatory mediators. Have the patient continue this therapy until the benefit is no longer realized, or use it PRN to maintain comfort. In our clinic, we recommend warming a wash cloth using hot water (as warm as the patient can stand, without burning the skin) and applying it simultaneously to both eyelids for five to 10 seconds. Then, we tell the patient to use one or two fingers to “stroke” the glands across both eyelids (e.g. from the distal extent of the tarsal plates toward the lash line.)
► Lipid replacement artificial tears. These products replace/supplement the missing lipids that should be normally secreted by the meibomian glands. While direct evidence is limited, lipid replacement should reduce the evaporation rate and should provide symptomatic relief and help to protect and possibly heal the ocular surface. Typical dosing is PRN, or up to six times a day (spread throughout the day) if the drop contains a preservative. (Preserved supplement used more than six times per day can begin to cause preservative medicamentosa in susceptible individuals.)
► Mid-viscosity aqueous lubricant. Mid-viscosity lubricants reduce inflammation by (1) washing out inflammatory cytokines and (2) providing a thicker, more stable tear film, which reduces the inflammatory stimulus. These products cause minimal blur and have effective residence times on the ocular surface (~ 25-35 minutes vs. saline at ~20 minutes).9 The typical dosage is PRN or up to six times a day (for the same reason given above.) Some patients find a drop at bedtime useful. There are two reasons for this: (1) Some dry eye patients are worse in the morning—for unknown reasons—and that group benefits by night drops. (2) There is no tear secretion at night, so patients with a very low aqueous can become very dry then.
► Omega 3 fatty acids. The metabolites of both Omega-6 and Omega-3 essential fatty acids (EFAs) are anti-inflammatory when the dietary ratio is 4:1. That said, the typical North American diet is closer to 15:1 causing the derivatives of the Omega-6 EFAs to contribute to the inflammatory process.10 To meet the aforementioned treatment goals, prescribe a fish-oil-derived (docosahexaenoic acid [DHA] and eicosapentaenoic acid [EPA]) Omega-3 FA supplement, 1g qd. Be sure to warn the patient of possible related GI-upset in the first two weeks of intake. Also, if the patient is using a blood thinner and/or serum lipid-lowering drugs, consult with his primary-care physician prior to prescribing, as omega 3 fatty acid supplements can add to these therapeutic effects. It may take one-to-two months of constant use to notice a marked effect of the supplement.
If the patient experiences no improvement with any of the aforementioned treatments, prescribe the following:
► The continuation of warm compresses and lubricants.
► An increase in omega 3 intake to 2g qd. after three months of no improvement with the 1g dosing.
► Moisture-chamber spectacles. Many studies have demonstrated that tear film stability and lipid layer appearance improve within 30 minutes of moisture chamber utilization.11
► Topical anti-inflammatory drugs (e.g., soft steroids [q.i.d.[, cyclosporine ophthalmic emulsion 0.05% (Restasis, Allergan, Inc.) [b.i.d.]). Have the patient use one of these drugs until inflammation subsides. Also, check baseline: optic nerve head, IOP and visual fields (glaucomatous signs) prior to initiation of therapy. Taper.
► Prescribe systemic tetracycline derivatives: The tetracycline derivatives are anti-inflammatory in action and when inflammation is reduced, the glands can secrete more and better quality lipids. The initial dose should be 50mg qd. for two weeks. Next, increase to 100 mg qd. Then, taper to 50mg qd. (Note: Therapy may need to be continued for three to six months in cases in which inflammation is not subsiding and/or symptoms are not improving.) Consider a maintenance dose of 20mg to 50mg qd. for long-term therapy. Warn the patient of possible stained teeth, photosensitivity and vaginitis.
Staging MGD severity
The recent MGD Workshop Report proposes an evidence-based approach to managing MGD. Specifically, the report consists of four stages (clinical descriptions) of MGD and the treatment protocol per stage. At each level of management, no response advances management to the next level. Certain portions of recommended management contain “+” (use your clinical judgment) or “+” (treatment is supported by the evidence at that disease stage). (See insert: “Meibomian gland dysfunction: what is it, why does it occur and how may it be treated?) While the staging concept is an important step forward in our ability to best manage these patients, and is vital to clinical trials and reimbursement, future research is needed to establish the validity and reliability of the specific sub-scales that comprise the severity assessment system.
The International Workshop on MGD reports are the most current literature on MGD. Overseen by more than 50 dry eye experts through a two-year period, these reports summarize the evidence-based knowledge we have to date regarding the diagnosis and management of this underrated condition. It will take time, but these research findings will result in improved knowledge of the mechanisms of disease development and, thus, greater understanding of effective management approaches. OM
1. The epidemiology of dry eye disease: report of the Epidemiology Subcommittee of the International Dry Eye Workshop (2007). Ocul Surf. 2007 Apr;5(2):93-107.
2. Nelson JD, Shimazaki, J, Benitez-Del-Castillo JM, et al. The international workshop on meibomian gland dysfunction: report of the definition and classification subcommittee. Invest Ophthalmol Vis Sci. 2011 Mar 30; 52(4):1930-7.
3. de Paiva CS, Lindsey JL, Pflugfelder SC. Assessing the severity of keratitis sicca with videokeratoscopic indices. Ophthalmology. 2003 Jun;110(6):1102-9.
4. Arita R, Itoh K, Maeda S, et al. Proposed diagnostic criteria for obstructive meibomian gland dysfunction. Ophthalmology 2009 Nov;116(11):2058-63.e1.
5. Pflugfelder SC, Tseng, SC, Sanabria O, et al. Evaluation of subjective assessments and objective diagnostic tests for diagnosing tear-film disorders known to cause ocular irritation. Cornea, 1998 Jan;17(1):38-56.
6. Bailey IL, Bullimore MA, Raasch TW, Taylor HR. Clinical grading and the effects of scaling. Invest Ophthalmol Vis Sci. 1991 Feb;32(2):422-32.
7. Korb DR, Black CA. Meibomian gland diagnostic expressibility: correlation with dry eye symptoms and gland location. Cornea 2008 Dec;27(10):p.1142-7.
8. Norn M. Meibomian orifices and Marx's line. Studied by triple vital staining. Acta Ophthalmol (Copenh). 1985 Dec;63(6):698-700.
9. Paugh JR., Nguyen AL, Ketelson HA, et al. Pre-corneal residence time of artificial tears measured in dry eye subjects. Optom Vis Sci. 2008 Aug;85(8):725-31.
10. Miljanovic B., Trivedi KA, Dana MR, et al. Relation between dietary n-3 and n-6 fatty acids and clinically diagnosed dry eye syndrome in women. Am J Clin Nutr. 2005 Oct;82(4):887-93.
11. Paugh JR, Meadows DL, Christensen M. The effect of increased periocular humidity on tear parameters. Poster presented at the American Academy of Optometry Meeting, San Diego, Calif. Dec 2002, OVS 79(12s): 252.

| Dr. Paugh is the Coordinator of the Dry Eye Institute at the Southern Californian College of Optometry and has contributed to the reports of both the Dry Eye and Meibomian Gland Dysfunction Workshops sponsored by the Tear Film and Ocular Surface Society. He has conducted numerous studies on dry eye diagnosis and management. Email him at jpaugh@scco.edu. Or, send comments to optometricmanagement@gmail.com. |