


infection
The Path of Least Resistance
By brushing up on the common bugs, the bug drugs and bacterial resistance development, you can delay it.
Andrew S. Gurwood, O.D., F.A.A.O., DIPL., Dayna R. Helvick, B.S.
Bacterial resistance is an unstoppable evolutionary mechanism. Yet, it is possible for eyecare practitioners to slow bacterial resistance by understanding the common microbes, the topical antibiotics and how, specifically, bacterial resistance develops.
Common microbes
There are many ways to classify bacteria. The primary method of dividing them is based on the physical properties of their cell wall (the amount of peptidoglycan). This is accomplished using the Gram stain. There are four basic steps of the Gram stain. (1) A colony of living organisms is prepared by heat-fixing (death by heat) them to a glass slide. (2) They are then soaked in the primary stain crystal violet. (3) After the excess primary stain is poured off, a trapping agent (Gram's iodine) is applied. (4) Finally, rapid decolorization is accomplished by introducing alcohol or acetone, and the final step of counter-staining with safranin is completed. Gram-positive bacteria have a thick cell wall with a large constituency of peptidoglycan, which stains purple. Gram-negative bacteria have a thinner cell wall with less peptidoglycan permitting them to give up the purple during the decolorization process and stain pink. Gram-negative bacteria also have an additional outer membrane that contains lipids.
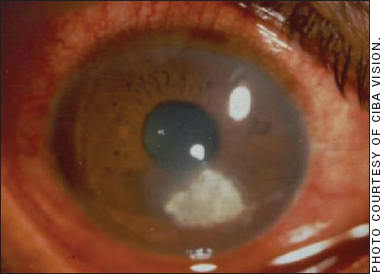
This patient has microbial keratitis (MK) due to contact lens wear. The most common microbe linked with contact lens-caused MK is Pseudomonas aeruginosa.
Although the bacteria Staphylococci (Gram-positive), Streptococci (Gram-positive), Corynebacterium (Gram-positive), Haemophilus (Gram-negative), Moraxella (Gram-negative) and Neisseria (Gram-negative) are part of the conjunctivae's normal flora, under appropriate conditions, they can overrun natural defenses to cause infection. (See “Mechanisms of Infection,” at the end.)
The most common bacteria isolated from ocular specimens are Staphylococcus aureus, followed by Streptococcus pneumoniae.1,2 S. aureus plays a role in infections of the eyelids, conjunctivae and canaliculi, whereas Streptococcus pneumoniae is more common in infections of the lacrimal sac, cornea and postoperative and post-traumatic endophthalmitis.3,4 Infectious blepharitis is typically caused by Staphylococcus and Moraxella.3,5 The bacteria most frequently linked with infectious conjunctivitis are Streptococcus pneumoniae, S. aureus, H. influenzae, Moraxella and Chlamydia trachomatis3,5 (Gram-negative). Severe mucopurulent bacterial conjunctivitis can be caused by Neisseria gonorrhoeae.6 Bacterial keratitis is normally caused by S. aureus, Streptococcus pneumoniae or S. epidermidis.1,6 Pathogens causing keratitis: Pseudomonas aeruginosa, S. aureus, S. epidermidis, Streptococcus pneumoniae and Moraxella.1,7
The bug drugs
The topical antibiotics are comprised of:
► Aminoglycosides. The topical aminoglycosides disrupt bacterial protein synthesis by binding to the 30S subunit of the bacterial ribosome and interfering with the formation of what is known as the initiation complex. This causes a misreading of the messenger ribonucleic acid.8Ribosomal ribonucleic acid (rRNA) is the component of the ribosome—the organelle that is the site of protein synthesis in all living cells. Ribosomal RNA (rRNA) provides the mechanism for decoding mRNA into the necessary amino acids for life and interacts with transfer RNA by providing peptidyl transferase activity.9 (See “Topical Aminoglycosides,” at the end.) By interrupting these processes inside the bacterial cells, their viability is altered.
► Fluoroquinolones. The most obvious difference between human and bacterial cells is that bacterium has a single chromosome without a nuclear membrane, which consists of a tightly wound super-coiled DNA molecule lying within the bacterial cytoplasm.10 Enzymes control the uncoiling and recoiling of the chromosome so that replication functions can occur. DNA gyrase maintains DNA super-coiling tension, which is essential for DNA replication and transcription.11 Topoisomerase IV uncoils circular DNA chromosomes, which is essential for chromosome segregation.12 The fluoroquinolones disrupt the super coiling of the bacterial chromosome by inhibiting the last step in peptidoglycan synthesis.11 Specifically, these antibiotics block bacterial growth by forming enzyme-fluoroquinolone-DNA complexes with two of the essential enzymes involved in bacterial DNA synthesis (DNA gyrase and topoisomerase IV).12,13 (See “Topical Fluoroquinolones,” at the end.)
► Macrolides. The topical marcolides disrupt bacterial protein synthesis by binding to the 23S rRNA molecule in the 50S subunit of the bacterial ribosome where they block the elongation of the growing peptide chain.9 (See “Topical Macrolides,” at the end.)
Although topical antibiotics can disrupt the architecture and function of bacteria cells, it is clear that evolution has given them the ability to evolve quickly to manifest resistance to pharmaceutical attacks.
Bacterial resistance development
Antibiotic resistance occurs when bacteria acquire genes that allow them to interfere with an antibiotic's mechanism of action either through spontaneous DNA mutation, transformation or transfer of plasmids.14 These resistant cells multiply creating strains of resistant organisms known as super infections.14
All bacterial resistance to antibiotics occurs in the following ways:
► The inactivation of the antibacterial agent before it enters the bacterial cell.
► The impermeability of the bacterial cell wall and plasma membrane to the anti-bacterial agent. The topical aminoglycosides have been susceptible to this bacterial resistance.15
► The development of a pumping mechanism for extruding the antibacterial molecules (efflux) from its cell.16 The topical fluoroquinolones have been susceptible to this bacterial resistance. Bacterial resistance to the fluoroquinolones developed when various bacterial organisms created alterations in their target enzymes. Alterations in target enzymes included mutations associated with DNA gyrase, which occurred in fluoroquinolone-resistant Gram-negative bacteria or mutations in topoisomerase IV.10,15 These alterations denied access to the enzymes targeted by fluoroquinolones, preventing them from crossing the bacterial cell wall.16
► The alteration of the “target” enzyme within the bacterium. Topical macrolides are susceptible to this bacterial resistance.14 Specifically, a recognition site no longer exists for the antibacterial agent to act upon.17
► The development of an alternative metabolic pathway to the antibacterial when it has reached and attempted to disable the metabolic target.
In general, four courses of action on our part help kick start bacterial resistance development: (1) the unnecessary use of topical antibacterial medicines for self-limiting, non-infectious conditions and viral infections; (2) selecting the wrong agent; (3) prolonged courses of treatment; and (4) tapering to a dosage less than the FDA-recommended minimum for a specific agent.18 Therefore, to slow bacterial resistance to topical antibiotics we must employ these drugs only when a reasonable potential for efficacy exists.18
Signs of ocular infection include conjunctival redness, the appearance of mucopurulent discharge, variable punctate keratitis, conjunctival follicles, conjunctival papillae and swollen preauricular, sublingual or submandibular lymph nodes. While lymph nodes are a sign of viral infection, they can certainly be involved in bacterial infection. Swollen lymph nodes without the constellation of the other signs indicative of bacterial infection may be indicate viral infection, in which case a topical antibiotic will have little action.
Today, it is uncommon to culture infectious conjunctival material to identify the offending pathogen. In several cases, empirical use of topical fourth-generation antibiotics are successful for eradicating the offending pathogen. It is important to employ high concentrations of the drug through a period of time such that all infectious microbial colonies are eradicated. In this light, patients should be instructed to finish the prescribed course of treatment and to not skip doses.18 Finally, we must not taper antibiotics (unless instructed to do so by the drug manufacturer), as tapering provides the pathogen with an opportunity to build up its defenses against a drug.
The management of bacterial ocular infection using topical antibiotics is dependent on the timely identification of infection and the selection of an appropriate medication to achieve eradication of the invading organism. Resistance to topical antibiotic treatment can be delayed by reacquainting yourself with the common pathogens, the topical antibiotics and the development of bacterial resistance to these drugs. OM
1. Ramesh S, Ramakrishnan R, Bharathi M, et al. Prevalence of bacterial pathogens causing ocular infections in South India. Indian J Pathol Microbiol. 2010 Apr-Jun;53(2):281-6.
2. Callegan M, Ramirez R, Kane S. Antibacterial activity of the fourth-generation fluoroquinolones gatifloxacin and moxifloxacin against ocular pathogens. Adv Ther. 2003 Sep-Oct;20(5):246-52.
3. Harris G, Kersten R, Codere F, et al. Orbit, Eyelids, and Lacrimal System, American Academy of Ophthalmology. Section 7. San Francisco, CA. Lifelong. 2007.41-47.
4. Karpecki P, Paterno MR, Comstock TL. Limitations of current antibiotics for the treatment of bacterial conjunctivitis. Optometry and Vision Science. 2010;87(11): 908-919. Optom Vis Sci. 2010 Nov;87(11):908-19.
5. Verma V, Shen D, Sieving PC et al. The Role of Infectious Agents in the Etiology of Ocular Adnexal Neoplasia. Surv Ophthalmol. 2008;53(4):312-31.
6. Tipple C, Smith A, Bakowska E, et al. Corneal perforation requiring corneal grafting: a rare complication of gonococcal eye infection. Sex Transm Infect. 2010;86(6):447-8.
7. Sherwal B, Verma A. Epidemiology of Ocular Infection Due to Bacteria and Fungus–A Prospective Study. JK Science. 2008;10(3):127-131.
8. Morden NE, Berke EM. Topical Fluoroquinolones for the Eye and Ear. Am Fam Physician. 2000;62(8):1870-6.
9. Yolton DP, Haesaert SP. Anti-Infective Drugs. In : Barlett J, Janus S. Clinical Ocular Pharmacology. New York, NY, Elsevier Health Sciences 2008:176-182.
10. Tenover FC. Mechanisms of antimicrobial resistance in bacteria. Am J Infect Control. 2006 Jun;34(5 Suppl 1):S3-10.
11. Senthilkumar P, Dinakaran M, Yogeeswari P, et al. Antimycobacterial activities of novel fluoroquinolones. Biomed Pharmacother. 2009 Jan;63(1):27-35. Epub 2007 Oct 29.
12. Labetoulle M, Chiquet C. Fluoroquinolones in ophthalmology: mechanisms of action and resistance. Journal of Ophthalmology. J Fr Ophtalmol. 2008 Oct;31(8):795-801.
13. Watanabe R, Nakazawa T, Yokokura S, et al. Fluoroquinolone antibacterial eye drops: effects on normal human corneal epithelium, stroma, and endothelium. Clin Ophthalmol. 2010 Oct 21;4:1181-7.
14. Abelson M, Pliumer A. Bacterial Resistance: The Ubiquitous Menance. Review of Ophthalmology. 2004;11(11):17-21.
15. Ness T. Multiresistant bacteria in Ophthalmology. Ophthalmologe. 2010 Apr;107(4):318-22.
16. Kaye S, Tuft S, Neal T, et al. Bacterial susceptibility to topical antimicrobials and clinical outcome in bacterial keratitis. Invest Ophthalmol Vis Sci. 2010 Jan;51(1):362-8.
17. Akpek EK, Gottsch JD. Immune Defense at the Ocular Surface. Eye. 2003 Nov;17(1):949-956.
18. Behrens-Baumann W, Frank U, Ness T. Rational antibiotic therapy in ophthalmology. Ophthalmologe. 2010 Apr;107(4):323-7. German.
19. Davis H, Mant D, Scott C, et al. Relative impact of clinical evidence and over-the-counter prescribing on topical antibiotic use for acute infective conjunctivitis. Br J Gen Pract. 2009 Dec;59 (569):897-900.
20. Goldstein MH, Kowalski RP, Gordon YJ. Emerging fluoroquinolone resistance in bacterial keratitis: a 5-year review. Ophthalmology 1999 Jul;106(7):1313-1318.
21. Ince D, Zhang X, Hooper DC. Activity of and resistance to moxifloxacin in Staphylococcus aureus. Antimicrob Agents Chemother. 2003 Apr;47(4):1410-5.
22. Wise R. Maximizing efficacy and reducing the emergence of resistance. J Antimicrob Chemother. 2003 May;51 Suppl 1:37-42.
23. Chaudhry N. Emerging ciprofloxacin-resistant Pseudomonas aeruginosa. Am J Ophthalmol. 1999 Oct;128(4):509-10.
| Mechanisms of Infection |
|---|
| The establishment of an infection depends on the virulence of the pathogen (the larger the inoculum, the greater the likelihood of infection), the route of the introduction of the pathogen, the state of the host's defense (e.g. preexisting corneal or conjunctival pathology, such as chronic infections of the adjacent sinuses, eyelids or orbits, can cause structural and functional alterations that affect the normal tissue responses to injury, inflammation or infection3,19,20) and the host's immune response status.17 (Local or systemic immune system breakdown will leave the host vulnerable to infection.21) Also, persons with functionally abnormal leukocytes have demonstrated a predisposition to marginal keratitis and blepharoconjunctivitis secondary to an impaired ability to control normal flora.3,22 In addition, acquired defects in cell-mediated immunity occur with a variety of diseases, including AIDS, multiple myeloma, sarcoidosis and diabetes mellitus.14 Systemic infections—in particular measles and tuberculosis—depress cell-mediated immunity.21 Abnormalities in cell-mediated immune function are also found in elderly persons, neonates, drug-dependant individuals and patients on chemotherapy.15) The infection of ocular surface tissues requires the microorganism to attach, penetrate, invade and replicate within the conjunctival environment.10 (The adherence of some bacteria to ocular structures is enhanced by components of the bacterial cell wall, such as the pili of Pseudomonas that bind to epithelial glycoprotein.10,22) Most bacteria enter the tissue following the disruption of the eye's physical defenses. This can occur via accidental or surgical trauma, lagophthalmos, excessive friction from trichiasis and contact lens wear.5,14 Exotoxins and proteases are virulence factors that destroy host immune cells and tissue matrix.23 Proteases include streptolysin, produced by Streptococcus pyogenes and P. elastase, and alkaline protease. These molecules can destroy both tissue collagen and proteoglycans while degrading immunoglobulins, complement, interleukins, and inflammatory cytokines, making bacterial penetration possible.14,23 Some bacteria, such as Pseudomonas, secrete a protective extracellular polysaccharide glycocalyx that encase the colony, creating a biofilm that is resistant to immune clearance and antimicrobial drug effects.22 Biofilm formation is believed to play an important role in the pathogenesis of contact lens keratitis.10 |
| Topical Macrolides |
|---|
| ► Azithromycin ophthalmic solution 1% (Azasite, Inspire Pharmaceuticals). Dosing: Bacterial conjunctivitis: Days one and two: one drop b.i.d. eight to 12 hours apart. Days three through seven: one drop qd. Pediatric use: age one. Gram-positive bacteria: CDC coryneform group G*, S. aureus, Streptococcus mitis group and Streptococcus pneumoniae. Gram-negative bacteria: H. influenzae. ► Erythromycin ophthalmic ointment 0.5% (Ilotycin, Fera Pharmaceuticals, LLC). Dosing: Superficial ocular infections: a ribbon 1cm in length six times daily, depending on infection severity. For prophylaxis of neonatal gonococcal or chlamydial conjunctivitis, a ribbon 1cm in length into each lower conjunctival sac. Gram-positive bacteria: Streptococcus pyogenes (group A β-hemolytic), Alpha-hemolytic streptococci (viridans group) Corynebacterium diphtheriae, S. aureus, including penicillinase-producing strains (methicillin-resistant staphylococci are uniformly resistant to erythromycin), Streptococcus pneumoniae and Mycoplasma pneumoniae (Eaton Agent, PPLO). Gram-negative bacteria: H. influenzae (not all strains are susceptible at erythromycin concentrations ordinarily achieved), Treponema pallidum, Neisseria gonorrhoeae and Chlamydia trachomatis. * Efficacy studied in fewer than 10 organisms. |
| Topical Aminoglycosides |
|---|
| ► Garamycin ophthalmic ointment (gentamicin sulfate, Fera Pharmaceuticals). Dosing: Apply a small amount (about 1/2 inch) to the affected eye(s) b.i.d. to q.i.d. Pediatric use: N/A. Gram-positive bacteria: Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus pyogenes, Streptococcus pneumonia. Gram-negative bacteria: Enterobacter aerogenes, Escherichia coli, Haemophilus influenzae, Klebsiella pneumoniae, Neisseria gonorrhoeae, Pseudomonas aeruginosa and Serratia marcescens. ► Gentamicin sulfate ophthalmic solution 0.3 % (Genoptic, Allergan,Inc.). Dosing: one or two drops q4h. For severe infections, increase to two drops q1h maximum. Pediatric use: age one month. Gram-positive bacteria: Coagulase positive and negative Staphylococci. Gram-negative bacteria: P. aeruginosa, Indole positive and Indole negative Proteus species, E. Coli, Klebsiella pneumoniae, H. influenzae, H. aegyptius, aerobacter aerogenes, Moraxella lacunata and Neisseria species. ► Polymyxin B sulfate and trimethoprim ophthalmic solution, USP (Polytrim, Allergan, Inc.). Dosing: For mild to moderate infections, one drop q3h (six-dose maximum per day) for seven to 10 days. Pediatric use: age two months. Gram-positive bacteria: S. aureus, S. epidermidis, S. pneumoniae, Streptococcus viridans. Gram-negative bacteria: H. influenzae and P. aeruginosa. ► Neomycin/polymixin B and gramicidin ophthalmic solution USP (Neosporin Ophthalmic Solution, Monarch Pharmaceuticals, Inc.) Dosing: One or two drops q4h for seven to 10 days. For severe infections, increase dosage to two drops q1h. Pediatric use: N/A. Gram-positive bacteria S. aureus, Streptococci, including Streptococcus pneumonia. Gram-negative bacteria: E. coli, H. influenzae, Klebsiella/Enterobacter species, Neisseria species and P. aeruginosa. ► Polymyxin B sulfate and bacitracin zinc ointment (Polysporin, Monarch Pharmaceuticals). Dosing: Apply q3h to q4h for seven to 10 days, based on infection severity. Pediatric use: N/A. Gram-positive bacteria: S. aureus, Streptococci, including Streptococcus pneumoniae. Gram-negative bacteria: E. coli, H. influenzae, Klebsiella/Enterobacter species, Neisseria species and P. aeruginosa. |
| Topical Fluoroquinolones |
|---|
| ► Besifloxacin ophthalmic suspension 0.6% (Besivance, Bausch + Lomb). Dosing: Bacterial conjunctivitis: t.i.d. four to 12 hours apart for seven days. Pediatric use: age one. Gram-positive bacteria: Staphylococcus aureus, S. epidermidis, S. hominis*, S. lugdenensis*, S. mitis group, S. oralis, S. pneumoniae, Streptococcus salivarius* CDC coryneform group G, corynebacterium pseudodiphtheriticum* and corynebacterium striatum*. Gram-negative bacteria: Haemophilus influenzae and moraxella lacunata* ► Ciprofloxacin HCl ophthalmic solution 0.3% (Ciloxan, Alcon, Inc.). Dosing: Corneal ulcers: Day one: two drops every 15 minutes for the first six hours and then two drops every 30 minutes. Day two: two drops qh. Day three through 14: two drops q4h. (Treatment may be continued after 14 days if corneal re-epithelialization has not occurred.) Bacterial conjunctivitis: One or two drops into the conjunctival sac(s) q2h while awake for two days, and one or two drops q4h while awake for the next five days. Pediatric use: age one. Gram-positive bacteria: S. aureus, S. epidermidis, Streptococcus pneumoniae and Streptococcus [viridans group]. Gram-negative bacteria: H. influenzae, Pseudomonas aeruginosa and Serratia marcescens. ► Gatifloxacin ophthalmic solution 0.3% (Zymar, Allergan, Inc.). Dosing: Bacterial conjunctivitis: Days one and two: one drop q2h while awake up to eight times a day. Days three through seven: one drop q.i.d. while awake. Pediatric use: age one. Gram-positive bacteria: Corynebacterium propinquum*, S. aureus, S. epidermidis, Streptococcus mitis* and Streptococcus pneumoniae. Gram-negative bacteria: H. influenzae. ► Gatifloxacin ophthalmic solution 0.5% (Zymaxid, Allergan Inc.). Dosing: Day one: one drop q2h while awake, up to eight times. Days two through seven: one drop b.i.d. to q.i.d. daily while awake. Pediatric use: age one. Gram-positive bacteria: S. aureaus, S. epidermidis, Streptococcus mitis group*, Streptococcus oralis* and Streptococcus pneumoniae. Gram-negative bacteria: H. influenzae. ► Levofloxacin 1.5% (Iquix, Vistakon Pharmaceuticals, LLC.). Dosing: Days one through three: one-to-two drops every 30 minutes to two hours while awake and approximately four and six hours after retiring. Days four through treatment completion: one to two drops q1h to q4h while awake. Pediatric use: age six. Gram-positive bacteria: Corynebacterium species*, S. aureus and S. epidermidis. Gram-negative bacteria: P. aeruginosa and Serratia marcescens.* ► Levofloxacin 0.5% (Quixin, Vistakon Pharmaceuticals, LLC.). Dosing: Days one and two: one-to-two drops q2h while awake up to eight times per day. Days three through seven: one to two drops q4h while awake, q.i.d. Pediatric use: age one. Gram-positive bacteria: Corynebacterium species*, S. aureus, S. epidermidis, S. pneumoniae, Streptococcus (Group C/F), Streptococcus (Group G) and viridans group Streptococci. Gram-negative bacteria: Acinetobacter lwoffii*, H. influenzae and Serratia marcescens*. ► Moxifloxacin HCI ophthalmic solution 0.5% (Vigamox, Alcon, Inc.). Dosing: one drop t.i.d. for seven days. Pediatric use: age one. Gram-positive bacteria: Corynebacterium species*, Micrococcus luteus*, S. aureus, S. epidermidis, S. haemolyticus, S. hominis, S. warneri* Streptococcus pneumoniae and Streptococcus viridans group. Gram-negative bacteria: Acinetobacter lwoffii*, H. influenzae, H. parainfluenzae* Other microorganisms: Chlamydia trachomatis. ► Moxifloxacin HCI ophthalmic solution 0.5% (Moxeza, Alcon, Inc.). Dosing: one drop b.i.d. for seven days. Pediatric use: age four months. Gram-positive bacteria: S. arlettae*, S. aureus, S. capitis, S. epidermidis, S. haemolyticus, S. hominis, S. saprophyticus*, S. warneri*, Streptococcus mitis*, S. pneumoniae, Streptococcus parasanguinis*, Aerococcus viridans, Corynebacterium macginleyi*, Enterococcus faecalis* and micrococcus luteus*. Gram-negative bacteria: E. coli*, H. influenzae, Klebsiella pneumoniae*, Propionibacterium acnes and Chlamydia trachomatis*. ► Ofloxacin ophthalmic solution 0.3% (Ocuflox, Allergan Inc.). Dosing: Bacterial conjunctivitis: Days one and two: one to two drops q2h to q4h. Days three through seven: one-to-two drops q.i.d. Bacterial corneal ulcer: Days one and two: one-to-two drops every 30 minutes, while awake. Approximately four and six hours after retiring, one-to-two drops. Days three through seven to nine: one-to-two drops hourly, while awake. Days seven to nine through treatment completion: one-to-two drops, q.i.d. Pediatric use: age one. Gram-positive bacteria: S. aureus, S. epidermidis and Streptococcus pneumoniae. Gram-negative bacteria: Enterobacter cloacae, H. influenzae, Proteus mirabilis, P. aeruginosa and Serratia marcescens*. Other microorganisms: Propionibacterium acnes. * Efficacy was studied in fewer than 10 infections. |
| Dr. Gurwood is a professor at PCO at Salus University in Elkins Park, Pa. Ms. Helvick will graduate this spring and begin her residency in The William Feinbloom Vision Rehabilitation Center at The Eye Institute of The Pennsylvania College of Optometry at Salus University, Philadelphia. Send comments to optometricmanagement@gmail.com. |