


healthcare reform
Healthcare Reform Brings Opportunities and Risks
Learn what the Affordable Care Act means to you and your practice.
Damian M. May, Pharm.D., M.B.A. and Scott A. Shields, M.B.A.
Various elements of the “Affordable Care Act” (ACA)* may impact optometrists in the coming years, from patient access, reimbursement and opportunity perspectives. After reading this article, you should understand the opportunities presented by healthcare reform, and how upcoming changes can and will affect the practice of optometry.
The ACA represents the most far-reaching change in healthcare since Medicare was created in 1965. It contains a variety of experimental provisions, which the Obama Administration believes will achieve the goals of increasing coverage, improving health status and lowering system costs.
The ACA has multiple provisions that go into effect at various points, from those immediately effective upon the legislative signing to provisions that are effective in a staged manner and won't be fully implemented until 2014—or as late as 2020.
As with many laws, the legislation is only the first step. Many provisions of the ACA were left purposely vague, so Executive Branch agencies could create specific regulations for their areas of responsibility.
To add another layer of complexity, many of the regulations won't go into effect until after they've been made available to the public for comment. So, optometrists should be aware of “proposed” regulations and make their thoughts known. The American Optometric Association's advocacy efforts will help ensure the profession's voices are heard in a collective manner.
*In this article, we use “Affordable Care Act” and “ACA” to refer to both the Patient Protection and Affordable Care Act (PPACA), P.L. 111-148 signed on 23 March 2010, and the Health Care and Education Reconciliation Act (HCERA), P.L. 111-152, signed on 30 March 2010.
Changes in reimbursement and coverage
The primary focus of the ACA is the expansion of the number of Americans with health insurance, which will significantly impact optometrists. According to the Congressional Budget Office (CBO), the ACA will increase the insured population by approximately 32 million Americans, mostly by increasing access to Medicaid (by about 16 million) and by creating private health benefit exchanges (also by about 16 million).1
To help finance the increased numbers of insured Americans, beginning in 2014, individuals will be responsible for obtaining “minimum essential coverage” for themselves and their dependents or they'll be forced to pay a penalty.2 “Minimum essential coverage” includes coverage under government-sponsored programs, eligible employersponsored plans, plans in the individual market, certain grandfathered group health plans and other coverage as recognized by regulation.
Individuals whose employers don't offer minimum essential coverage, and whose household incomes are 133% to 400% of the federal poverty level (FPL), will qualify for federal subsidies to help pay insurance premiums or cost-sharing obligations under a plan they purchase through a health benefit exchange.
The following is a description of the insurance expansion via Medicaid and insurance exchanges.
Medicaid
Effective January 1, 2014, the ACA requires states to expand Medicaid coverage to individuals who are under 65 years of age, not pregnant, not entitled to Medicare Part A or Part B benefits, and whose income does not exceed 133% of the federal poverty level (FPL) ($29,726 for a family of four in 2011).3 Additionally, the Medicaid benchmark coverage needs to provide at least the essential health benefits.4
American Health Benefit Exchanges
The ACA created American Health Benefits Exchanges to help individuals and small businesses find and enroll in private or public health insurance coverage. Access to the exchanges is limited to qualified employers and individuals, citizens and lawfully present immigrants.5 The ACA requires the benefit packages of plans offered in the exchanges to provide, at a minimum, essential health benefits (described below).
Essential Health Benefits
The ACA has mandated that, effective January 1, 2014, most health plans provide a standard minimum benefit package, called “Essential Health Benefits.”6 Essential health benefits must be provided by individual and small group health plans, as well as by any qualified health plan sold in the state exchange market. The provision is designed so that individuals have adequate coverage for a range of specific services when they purchase insurance. Some of the essential health benefits are fairly obvious choices, such as emergency services and hospitalizations. For optometrists, the most important benefit is providing “pediatric services, including oral and vision care.”7
As addressed earlier, the essential health benefit concept has two components: the enabling legislation (ACA), and the implementing regulations. While the ACA lists broad categories of essential health benefits, the implementing regulations specifying the exact components have yet to be written. Therefore, no one knows the composition of pediatric vision services that will be included as essential health benefits—whether they will include annual exams, materials provisions, fittings, and so on. CMS may issue proposed regulations, which will be available for comment, on essential health benefits later this year.
The regulations for essential health benefit will dictate the minimum level of services optometrists can provide to many privately insured Americans.
Sustainable Growth Rate
A notable missing ingredient to healthcare reform was eliminating or modifying the Medicare sustainable growth rate (SGR) payment methodology for providers. The SGR is designed to ensure that the yearly increase in the expense per Medicare beneficiary doesn't exceed the growth in gross domestic product.8 The SGR formula, however, begins to trim provider payments once healthcare costs exceed general growth in the economy. The spiraling increase in healthcare costs has resulted in Congressional intervention 13 times since 2002 to stave off Medicare payment cuts to providers.9 Barring additional intervention, the SGR will call for 29.5% Medicare payment cuts to providers beginning January 1, 2012.10
The SGR formula is widely seen as flawed, and Republicans in the House of Representatives are holding a series of hearings to explore opportunities to replace the SGR formula with a variety of Medicare payment options, including some models being tested now, such as accountable care organizations (ACOs), bundled payments, medical homes and shared decision-making.
Access to providers Harkin Amendment
One opportunity for optometrists to increase access to patients and payers is to expand their list of services, and the ACA may have opened that door. The so-called “Harkin Amendment” component of the ACA bars health insurers from discriminating in plan coverage and participation against optometrists and other providers.11 As a result, effective January 1, 2014, optometrists will have a new opportunity to be reimbursed for providing the entire suite of services for which they are scoped and licensed. This should help increase revenue per patient.
Moreover, if optometrists can provide their services in a more cost-effective manner, increased patient volume could result as patients and payers recognize value.
Mandates May Force Resource Decisions
A potential downside of the essential health benefit package is that, due to the large number of mandates, health plans and employers may have to make difficult decisions about how to resource the mandates and other benefits, which may result in certain benefits, such as vision care for adults, being dropped.
This possibility, however, is not as grave as it appears. The ACA allows “children” to remain on a parent's health plan until age 26, regardless of financial dependency on the participant or primary subscriber, residency with the participant or primary subscriber, student status, employment, eligibility for other coverage, or marital status.12 As a result, previously uninsured young adults will have health insurance through their parents, while insured young adults will have a choice between their individual health plan options and their parents' plans.
A contrasting school of thought is that, for a plan to maintain market share in a more competitive marketplace with the same standard of basic coverage, plans will actually be incentivized to add benefits beyond essential health benefits (e.g., adult vision care) to differentiate and to attract patients. A similar phenomenon existed in the airline industry before deregulation; with many factors controlled by the government, airlines could only compete on a limited number of factors, such as food. As a result, a point of differentiation was the quality of meal service on an airline. Some think the same marketing strategy might apply to health plans.
Medicare shared savings
As the inclusion of the Harkin Amendment represents the crowning achievement of healthcare reform for optometrists, the exclusion of optometrists from serving as principals in the Medicare Shared Savings Program (MSSP) is the nadir.
The MSSP is a Medicare program that relies on the ACO model to generate and to distribute savings. In an ACO model, a group of providers assume responsibility for a defined set of patients with the goal of achieving higher quality care while managing the costs of patient care under a risk sharing agreement. In the case of the MSSP, for example, if an ACO succeeds in delivering highquality care, and reducing the cost of that care to below what would otherwise have been expected, it will share in the Medicare savings it achieves.
CMS has proposed that, for the MSSP, the only providers who can participate fully in ACOs—and thus realize any shared savings—are the specialties of general practice, family practice, internal medicine and geriatric medicine.13 Optometrists would still be able to contract with ACOs, but only to provide their services, and not to benefit from shared savings.
Of course, the MSSP/ACO proposed rule has come under great criticism by physician societies and policy think tanks, so the implementing regulations are likely to look quite different once finalized.
Perhaps due to the criticism of the ACO/MSSP's proposed rule, CMS announced a different type of ACO model, called the “Pioneer ACO,” in May 2011. The Pioneer ACO model will allow “provider groups experienced with providing coordinated care to move more rapidly from a shared savings payment model to a population-based payment model on a track consistent with, but separate from, the Medicare Shared Savings Program. And it's designed to work in coordination with private payers by aligning provider incentives.”14
In this environment, there may be more opportunities for optometrists to work as part of the care-giving team, and to demonstrate their role in ensuring healthy patient outcomes.
Treating uninsured and underinsured
As discussed previously, healthcare reform may provide health insurance to more than 30 million additional Americans, mostly by Medicaid expansion and new insurance exchanges. This expansion will create a new dynamic of patients, whereby optometrists may see their payment per transaction decrease, but with the possibility of more transactions.
Optometrists should, as a whole, see increased foot traffic from the newly insured, who will be seeking eye exams and other services that they were unable to purchase in the past. These new patients may be candidates to purchase goods (e.g., frames, lenses, contact lenses) and services (glaucoma treatment, laser or cataract surgery, where scoped to provide such services).
Increased use of health care by baby boomers
Whereas healthcare reform will increase healthcare consumption among traditional underutilizers, demographics and the aging process will increase healthcare consumption among the baby boomers, due to the physiological consequences of their aging. A number of studies have shown how baby boomers will impact health care.
By 2030, the number of adults in the United States who are 65 years old or older is expected to be almost double what it was in 2005, representing an increase from approximately 37 million older adults in 2005 to over 70 million in 2030.15 The number of those who are aged 80 and over is also expected to nearly double, from 11 million to about 20 million.15
The National Center for Health Statistics (NCHS) has shown that, consistently, those in the 65-74 and 75+ age groups have demonstrably greater prevalence of chronic diseases than those in the 18- to 64-year-old group.16 With greater numbers of people requiring care for chronic disease, of course, come tremendous financial strains on the health system. The most recent Medicare Trustees Report includes sobering data:
► Medicare Part A is estimated to be exhausted in 2024, 5 years earlier than was shown in the 2010 report
► Medicare Part B and Part D, though adequately funded currently, are expected to experience 7.5% and 9.7% growth, respectively, much faster than the 5.2% growth the Medicare Trustees project for the U.S. economy17
► To add fuel to the fire, the Medicare Trustees may have an overly optimistic outlook of the U.S. economy, as it has only averaged 2.4% growth in the last eight quarters.18
The increased prevalence of chronic conditions as one ages also applies to vision. NHCS found that vision problems increase as people age, as well:
As demonstrated in Figure 1, the prevalence of vision trouble in the 65-74 (10.3%) and 75+ (16.5%) cohorts significantly exceeded those aged 18-64 (7.6%).
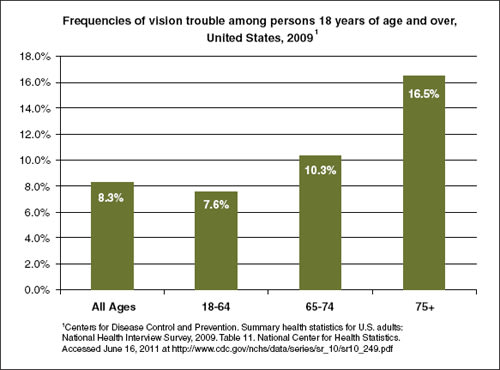
Figure 1. The prevalence of vision trouble in the 65-74 (10.3%) and 75+ (16.5%) cohorts significantly exceeded those aged 18-64 (7.6%).
How to prepare
So, how do you ensure that your practice remains profitable, increasing its efficiency and productivity, without compromising patient care? The Patient Protection and Affordable Care Act of 2010 will have a dramatic and long-standing effect on the American Health Care System, both in process and economics. These changes will drive many downstream behaviors that are fundamentally different from what is experienced in the current system. Patients will seek care and providers in a different, and one could argue, better funded way over the next decade. Insurers, both commercial and governmental, will need to better understand the dynamics of patient care seeking and purchasing behaviors in order to design products that both meet federally mandated standards and patient needs. Finally, all providers will experience a substantial change in the way in which patients enter their practices and pay for their care. Signing of the ACA legislation was a landmark achievement in the Obama Administration; however, it was simply the first step. There will continue to be many legal challenges to the constitutionality of the law and its mandates. There is much regulation to be written that will impact the ability to execute aspects of the Act. Finally, there is a larger funding exercise that will occur through appropriations and will determine exactly what resources will be available to drive these changes in the marketplace. Thus, there is much work to be done between now and January 1, 2014.
So, we ask ourselves, “What can be done today to prepare for this?” Between now and then, I would the profession, and individual doctors, to stay abreast of all political machinations associated with implementation of ACA. Regulations will be published for public comment. Ensure that your voice is heard—whether it be individually through direct contact with your member of Congress or collectively through the profession. Pay close attention to the 2012 elections, as the possibility of the Senate turning over to Republican control would substantially impact the ACA's implementation strategy and timelines.
Finally, stay mindful of the fact that the ACA is focused on a few primary issues. First, it is about access for patients who have impeded or minimal access today. This is important when one recognizes that optometry has much to offer in both routine care as well as preventive care. Optometry will be a critical piece of the provider landscape to ensure this access goal is met. Second, the act is about efficiency. Practices that figure out how to deliver the best care in the most cost-effective way will emerge as “winners.” Optometry has a tremendous opportunity to demonstrate that care delivered by the optometrist will meet the Obama Administration's goals of increasing coverage, improving health status and lowering system costs. Lastly, the act is about reforming reimbursement streams and ensuring that there is value for the dollar in health care. Much has been written about the high costs of health care in the United States and the relatively low health status those dollars generate. In the administration's view, this has to change through implementation and execution of ACA.
The future holds a bevy of opportunity and risk for all providers in health care. Optometry is certainly no different than any other provider group affected by the act. It will ultimately be up to the individual optometrist to best understand what value he adds to the system. Ensure that your practice is prepared for the challenge and well positioned to capitalize on the opportunities and manage the risks associated with this “new world” of healthcare delivery. OM
1. Elmendorf, D. Congressional Budget Office estimate sent to House Speaker Nancy Pelosi on the combined effects of the Patient Protection and Affordable Care Act and the reconciliation act, March. 20, 2010. www.cbo.gov/ftpdocs/113xx/doc11379/AmendReconProp. pdf.
2. ACA §1501(b).
3. ACA §2001.
4. ACA §2001(c).
5. ACA §1312(f).
6. ACA §1302.
7. ACA§1302(b)(1)(J).
8. Goldstein J. Why Medicare pay cuts for doctors will be back.Wall Street Journal Health Blog. July 10, 2008. http://blogs.wsj.com/health/2008/07/10/why-medicare-pay-cuts-for-doctors-willbe-back/.
9. Hann J. Medicare physician payment updates and the Sustainable Growth Rate (SGR) system. Congressional Research Service. August 6, 2010. http://aging.senate.gov/crs/medicare15.pdf
10. Lowes R. Physicians face 29.5% Medicare pay cut in 2012. Medscape Medical News. March 10, 2011. http://www.medscape.com/viewarticle/738753.
11. ACA §1201.
12. PPACA §1001, as modified by HCERA §2301(b).
13. 76 Fed Reg 19538.
14. CMS. Pioneer ACO Model. May 2011. Accessed June 22, 2011 at http://innovations.cms.gov/areasof-focus/seamless-and-coordinatedcare-models/pioneer-aco/.
15. Institute of Medicine. Retooling for an aging America: Building the health care workforce. 2008. Washington, DC: The National Academies Press.
16. Centers for Disease Control and Prevention. Summary health statistics for U.S. adults: National Health Interview Survey, 2009. National Center for Health Statistics. www.cdc.gov/nchs/data/series/sr_10/sr10_249.pdf.
17. 2011 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. May 13, 2011. www.cms.gov/ReportsTrustFunds/downloads/tr2011.pdf.
18. Bureau of Economic Analysis. US Department of Commerce. National income and product accounts Table 1.1.1. Percent change from preceding period in real Gross Domestic Product; 2009 to 2011. Accessed June 22, 2011 at www.bea.gov/national/nipaweb/TableView.asp?SelectedTable=1&ViewSeries=NO&Java=no&Request3Place=N&3Place=N&FromView=YES&Freq=Qtr&FirstYear=2009&LastYear=2011&3Place=N&Update=Update&JavaBox=no
19. Centers for Disease Control and Prevention. Summary health statistics for U.S. adults: National Health Interview Survey, 2009. Table 11. www.cdc.gov/nchs/data/series/sr_10/sr10_249.pdf.
| Damian M. May, Pharm. D., MBA, is Director of Managed Markets at Vistakon, a division of Johnson & Johnson Vision Care, Inc. Scott A. Shields, MBA, is Associate Director of Health Policy at Xcenda. |