


DRY EYE REPORT
Pinning Down Dry Eye
Take a 10-step approach to help ensure a complete diagnosis.

By Kelly K. Nichols, OD, MPH, PhD
Diagnosing dry eye disease is essential for many reasons — most importantly, to optimize patients' ocular health. Dry eye diagnosis and treatment are also part of the medical model of optometric practice, and they provide a good revenue stream (and keep you from losing dissatisfied patients).
Despite this, some optometrists don't routinely diagnose and treat dry eye disease. Here's what they're missing: Dry eye diagnosis and treatment are current standard of care for optometry.
In this article, I'm revisiting the 10-step concept presented by Scot Morris, OD, FAAO, in Optometric Management in 2008. He and I talked about how much things have changed in 3 years, including the standard of care for dry eye. In our profession, we've become more aware of ocular surface disease conditions, grown in our ability to manage it, gained more drug options, written more prescriptions, and adopted more dry eye subspecialties and clinics into our practices. Here are 10 steps to ensure you catch all of the dry eye sufferers in your practice.
STEP 1: Get it in their own words
I want to hear patients describe how their eyes feel in their own words, so I ask them if they ever have any eye discomfort, and if so, I tell them to describe their worst symptoms. They usually provide a descriptive word (itchy, gritty, and so on) that I can record and inquire about during their next visit.
This description also leads into a detailed, informative conversation. What time of day does the problem occur? Has the patient tried to treat it? If so, with what? Was the treatment successful? Has the problem improved or worsened? What activities does it affect (for example, driving or wearing contact lenses)?
A good in-office survey can also bring problems to your attention and help you begin asking the right questions, but if you discuss patients' problems and listen attentively to their answers, you should be able to obtain a complete, accurate picture.
STEP 2: Know their medications
Patients are often taking systemic medications that cause or influence ocular surface symptoms. If you see that a patient is taking oral antihistamines, beta-blockers, diuretics, or any other medication that has a side effect of dryness, then medication is likely contributing to the patient's dry eye symptoms.
Other medications, such as some drugs taken for rheumatoid arthritis, actually benefit the eyes, so a patient may find that symptoms improve or worsen when their rheumatologist changes their therapy. I've seen this occur with Sjögren's Syndrome sufferers. If the patient is taking supplements (for example, fish or flax oil), they may influence the ocular surface as well.
For more information on systemic medications and how they may affect the eyes, see ”Are Medications the Culprit?“.
STEP 3: See the ”big picture“ view
Patients' medications are one part of the big picture of their overall health. The medical history form should tell you all of the patients' past eye problems, including trauma, surgery or allergies, as well as other diagnosed health problems, such as diabetes and rosacea, that may affect the ocular surface. If these conditions aren't well controlled, you may need to work with the patient's primary care physician or make a referral.
In some cases, patients may be unaware of their existing health problems, so these conditions go unreported on their in-office history forms. To combat this problem, when I walk into the exam, I look at the patient's skin and joints for signs of inflammation. I observe the blink rate and eyelid closure while blinking, and I note the general appearance of the lid margins and conjunctiva. This initial once-over tells me a lot about the patient's overall health and possible causes of dry eye.
STEP 4: Follow a diagnostic routine
Use a standard routine to check for all ocular surface diseases. First, check the lids for signs of blepharitis or chronic inflammation. Most ocular surface diseases involve the lid margin, and the bulk of patients with evaporative dry eye have a lid disease such as meibomian gland dysfunction (MGD). (For more information on MGD, see ”Staging Meibomian Gland Disease“). Next, check the conjunctiva for hyperemia and follicles or papillary changes that may indicate infectious or inflammatory disease. Finally, observe the cornea without staining for dystrophies or irregularities. With the patient history, discussion, and standard exam complete, testing will help confirm or rule out any suspected problems.

Figure 1. Lissamine green staining in a patient with contact lens-related dry eye, likely with an MGD component.
STEP 5: Check tear film osmolarity
In this relatively new step, you can measure a core mechanism in dry eye disease using the TearLab Osmolarity System (TearLab Corporation). The instrument rates tear osmolarity (concentration) when a small tear sample is taken by bringing the tip to the inferior tear meniscus for a brief second or two. If the patient has a high value (greater than 308mOsm/Kg), then she is likely to have dry eye. If the numbers are in the mild to moderate range (305-320), use the number from the higher value of the two eyes to guide treatment decisions.
There is some variability in tear osmolarity testing that is related to variation in the tears of a patient, not the instrument, so when you schedule a follow-up visit to assess how dry eye treatment is working, choose the same time of day as the baseline exam. It might also be best to measure patients with symptoms but no other clinical signs at the end of the day, or when symptoms are worst. Remember to always make a note of the highest (worst) value of the two eyes — that is, the osmolarity measure that the ocular tear and surface ”system“ is capable of achieving.
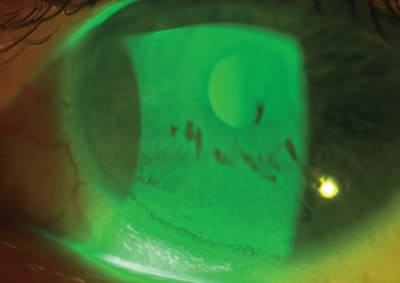
Figure 2. Inferior corneal staining with visible tear break-up time in a chronic dry eye patient.
STEP 6: Observe the meibum
MGD and other meibomian gland problems are part of most ocular surface diseases. Patients with MGD often complain of morning symptoms, including crusting of the eyelashes, puffy eyelids and red eyes. While symptoms may improve during the day, many patients report frequent blinking to clear their vision (for example, while watching TV at night).
Check for lid margin problems or blocked glands. Next, express the glands in both eyes and observe the quantity (Can you get any?) and quality (What color is it?) of the secretions. Is it clear (grade 0), slightly cloudy (grade 1), cloudy with a few particles (grade 2), granular and cloudy (grade 3), or white (toothpaste like, grade 4)?
STEP 7: Perform stains and test tear breakup
Vital dyes reveal any damage to the ocular surface caused by dry eye, while tear breakup time can tell us if the patient has problems like a heavy or contaminated lipid layer, insufficient aqueous-mucin gel layer, or a faulty or absent glycocalyx. Because lissamine green stain can affect tear break up testing, I do fluorescein staining first with a Wratten yellow filter, then tear breakup testing time, and finally lissamine staining.
A new combination fluorescein/lissamine dye called Fluramene (Noble Vision Group) is gaining popularity. Some doctors already use fluorescein and lissamine strips together, wetting them with saline. Regardless of the approach you take, always wait a minute or two for the best staining effect.
STEP 8: Evaluate tear volume
Schirmer's testing and the phenol red thread test are both good ways to evaluate the tear volume. A Schirmer's value below 5mm is most severe, possibly indicating Sjögren's. Patients with mild to moderate dry eye range from 5mm up to the normal cutoff of 10-15mm/5 min. Patients above 15mm are likely to be normal. Remember that the test becomes more variable as the numbers approach normal levels. I like to say that without treatment, a dry eye (<5mm) is going to be dry the next time you measure it. Therefore, you really should measure tear production at the first dry eye exam. Many doctors choose not to measure it every time, especially if the baseline numbers are in the normal or high borderline range.
If you worry you might lose patients by performing a Schirmer's test, consider the phenol red thread test, which is more patient friendly because it's less irritating and takes about 15 seconds per eye instead of 5 minutes (also blot the eyes or wait a minute or two after dye instillation). Then have the patient dab and remove the dye. At least once, the first time you see a patient with complaints, you should perform this test (or the Schirmer's test) to evaluate if your patient is aqueous deficient. Consider a rheumatology consult if your patient is female, has dry mouth, or has arthritis to rule out Sjögren's syndrome.
STEP 9: Test aqueous outflow
Aqueous outflow problems are not common and are usually unilateral, but if you suspect there may be a problem, the Jones test or irrigation will give you an answer. Unilateral or bilateral epiphora could be caused by blocked drainage. Some patients have reduced outflow in both eyes, usually because of the position of the puncta. Loss of lid elasticity may be a culprit as well, so be sure to evaluate the position of the lid against the eye.
STEP 10: Put it all together
At this point, you have a very clear picture of your patient's ocular surface problem and a good idea of the cause or causes. Design a treatment plan. Emphasize the importance of adhering to the plan, and schedule a follow-up visit in 6 to 8 weeks. This gives patients time to form the habit of using new drops or performing lid scrubs and warm compresses, but it doesn't give them time to fall off the wagon.
During the next visit, use your baseline series of tests to look for improvements. Listen to any complaints about the therapy and consider alternatives (if it's inconvenient, patients probably won't stick with it). I tell my patients that we're in it together, and we'll continue to work on the issue for as long as it takes. Patients can see the differences in their tests and photos, and that, along with increased comfort, validates our efforts to combat their dry eye.
Dr. Nichols is professor at the University of Houston College of Optometry in Houston, Texas.