


RESEARCH IN PRACTICE
Upper Punctal Occlusion
A recent study shows this method provides enhanced visual stability.

MILE BRUJIC, O.D., CRYSTAL BRIMER, O.D.
Clinically, we oftentimes occlude the lower puncta first, measure clinical outcomes and, if needed, occlude the upper puncta as well.
The study we discuss here questions this convention.
Supporting research
The study reveals that symptomatic dry eye disease (DED) patients who underwent upper punctal occlusion vs. lower punctal occlusion achieved greater visual stability.1
Specifically, 43 symptomatic DED patients were randomized to have either the lower puncta (24 patients) or upper puncta (19 patients) OD occluded. All patients had a tear break-up time (TBUT) of equal to or less than five seconds.
Also, the researchers measured their ocular surface fluorescein staining using the Japanese dry eye diagnostic criteria (e.g. the ocular surface is divided into the nasal conjunctiva, the cornea and the temporal conjunctiva). Fluorescein staining is graded in each area from 0 to 3, with 3 being maximal area staining and a maximum ocular surface score of 9. This study’s patients had a total ocular surface fluorescein staining score of less than 3 — minimal DED ocular signs.
The majority of patients in each group (17 of 19 in the upper punctum group and 19 of 24 in the lower punctum group) reported symptom resolution. Also, fluorescein surface staining scores decreased, and TBUT decreased in each group post-one month. That said, only eyes that underwent upper punctal occlusion experienced a significant improvement in the mean logarithm of the minimum angle of resolution functional visual acuity value.
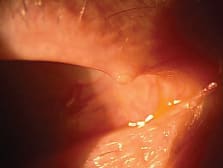
Upper punctal occlusion, shown here, appears to afford better visual stability in symptomatic dry eye disease patients vs. lower punctal occlusion, a recent study reveals.
Implications for patient care
Due to gravitational forces, it seems logical to initially occlude the lower puncta to optimize therapeutic success. However, studies show the amount of tears that drain through the superior and inferior canaliculi are relatively similar.2,3 In this study, patients who had their upper punctum occluded had greater visual stability than those who had lower punctum occlusion.
This is an interesting finding that we should take into account when treating our DED patients.
Of course it is worth noting that this study does have a limitation: The patients were not utilizing any DED medications. Thus, the results cannot necessarily be extrapolated to patients who may have been using topical steroids or cyclosporine ophthalmic emulsion 0.05% (Restasis, Allergan), but certainly may warrant further study for this group of patients. OM
1. Kaido M, Ishida R, Dogru M, Tsubota K. Visual function changes after punctal occlusion with the treatment of short BUT type of dry eye. Cornea. 2012 Sep; 31(9): 1009-13.
2. Murgatroyd H, Craig JP, Sloan B. Determination of relative contribution of the superior and inferior canaliculi to the lacrimal drainage system in health using the drop test. Clin Experiment Ophthalmol. 2004 Aug;32(4):404-10.
3. White WL, Glover AT, Buckner AB, Hartshorne MF. Relative canalicular tear flow as assessed by dacryoscintigraphy. Ophthalmology. 1989 Feb;96(2):167-9.
DR. BRUJIC IS A PARTNER OF PREMIER VISION GROUP, A FOUR-LOCATION OPTOMETRIC PRACTICE IN NORTHWEST, OHIO. HE HAS A SPECIAL INTEREST IN GLAUCOMA, CONTACT LENSES AND OCULAR DISEASE MANAGEMENT OF THE ANTERIOR SEGMENT. E-MAIL HIM AT BRUJIC@PRODIGY.NET.
DR. BRIMER OWNS CRYSTAL VISION SERVICES, AN OPHTHALMIC EQUIPMENT AND PRACTICE MANAGEMENT CONSULTING COMPANY. SHE PRACTICES IN WILMINGTON, NC AND HAS A SPECIAL INTEREST IN CONTACT LENSES AND DRY EYE MANAGEMENT. E-MAIL HER AT DRBRIMER@CRYS TALVISIONSERVICES.COM, OR SEND COMMENTS TO OPTOM ETRICMANAGEMENT@GMAIL.COM.