


CLINICAL
specialty care
Lowering IOP With Stents
When should you consider referring glaucoma patients for MIGS?
JUSTIN SCHWEITZER, O.D., SIOUX FALLS, S.D.
When many of us hear “MIGS,” we think of the Russian fighter jets in the ’80s blockbuster Top Gun: “Maverick, move! There’s a MiG on your tail!” Today in eye care, the term refers to Minimally Invasive Glaucoma Surgery, which is an innovative procedure designed for cataract surgery patients who have mild to moderate open angle glaucoma (OAG).
Here, I discuss this surgery in greater detail and provide the reasons you should consider referring your glaucoma patients for it.
MIGS defined
This procedure is comprised of inserting a single stent and, at times, multiple stents through the same clear corneal incisions used during cataract surgery to serve as a bypass through the trabecular meshwork. This allows physiological outflow and, therefore, lower intraocular pressure (IOP). (See figure 1.)
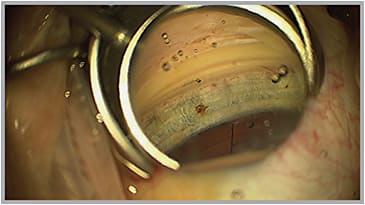
Figure 1: MIGS implanted through a clear corneal incision, through the trabecular meshwork into Schlemm’s canal with the assistance of a gonioprism. (Image courtesy of John Berdahl, M.D.)
The stent is contraindicated in patients with primary or secondary angle closure glaucoma, neovascular glaucoma and angle abnormalities, such as peripheral anterior synechia.
Adverse effects of insertion of stents include postoperative hyphema, IOP spikes and, uncommonly, peripheral anterior synechia to the stent.
A postoperative hyphema is not uncommon, and patients will complain of cloudy vision. Patient education is of utmost importance to reassure them that the hyphema will clear, usually within a week.
IOP spikes can occur due to retained viscoelastic or a delayed steroid response. Revising the tapering of the steroid can be beneficial in getting IOPs back to a normal level.
Specifically, adding glaucoma drops until IOPs have stabilized and then tapering patients off of those medications will help control these spikes. It is not uncommon for IOPs to fluctuate for the first three months postoperatively, and educating patients on these fluctuations will ease their concerns.
For your consideration
The four reasons you should contemplate referring your glaucoma patients for MIGS:
1. Safety. MIGS performed at the same time as cataract surgery has a greater safety profile than traditional filtration surgeries in combination with cataract surgery. Specifically, studies have demonstrated that MIGS performed along with cataract surgery do not compromise visual outcomes or the safety of the cataract procedure.
In contrast, traditional filtration surgeries place patients at risk for complications, such as bleb leaks, bleb infections or hypotony. In addition, studies reveal that filtration surgeries can induce corneal curvature changes, which adversely affect postoperative visual acuity. These complications are not a concern for patients implanted with glaucoma stents.
2. Increased compliance with glaucoma medications. A complex glaucoma-dosing regimen is difficult for patients to adhere to and, as a result, they are more likely to be non-complaint to it. Cataract surgery in combination with MIGS helps to decrease the number of glaucoma medications a patient is prescribed, therefore making compliance more likely.
3. Effectiveness. The procedure lowers IOP, thus protecting glaucoma patients from further disease progression, which leads to blindness. In fact, studies in Ophthalmology and the Journal of Cataract and Refractive Surgery reveal that 66% of eyes treated with cataract surgery and a glaucoma stent achieved a greater than 20% reduction in IOP without medications vs. 48% of eyes treated with cataract surgery alone, says a study in Ophthalmology.
The same studies reported that twice as many patients in the surgery-only group returned to medications at one year compared with those patients in the cataract surgery and glaucoma stent group. Further, the cataract surgery and glaucoma stent group showed an additional 3mmHG of IOP reduction compared with the surgery-only group. Finally, 15 months postoperatively, 67% of the cataract surgery and glaucoma stent group were medication free compared with 24% of the cataract surgery-alone group.
4. Affordability. Medications can become a financial burden for many patients, especially ones that are needed long term. No recent studies compare the current costs of these medications.
However, past studies reveal an average cost per year that varied between $400 and $600 dollars on monotherapy treatment. That cost increases as adjunctive therapy becomes necessary.
A direct cost comparison at six years of treating glaucoma patients with a MIGS device vs. bi-drug and tri-drug topical medications reveal a modest cost savings for patients in favor of the MIGS device. Specifically:
• $1,272.55 cumulative cost savings per patient for MIGS device vs. bi-drug.
• $2,124.71 cumulative cost savings per patient for MIGS device vs. tri-drug.
Preserving vision and doing what is best for the patient is the most important consideration when making treatment choices, no matter the cost. If treatment options exist that are superior or equally effective and cost the patient less, they should be considered.
In addition to the cost savings for patients, factors, such as quality of life and ocular surface issues, that arise with topical glaucoma medications make the role of MIGS in the treatment paradigm of glaucoma valuable. Patients who suffer from ocular surface disease secondary to glaucoma medications have a daily burden placed on them. If we are able to provide them with treatments to control their glaucoma and reduce the burden of ocular surface disease, they must be considered.
Coding
MIGS can present administrative personnel at ophthalmology practices with coding challenges. Implantation of a MIGS device is described by CPT code 0191T, a category III code or new technology code. Category III codes do not have global periods assigned to them, and insurance carriers will not currently recognize modifier -54 or -55 with 0191T. Modifier -54 and -55 can be applied to CPT code 66984 (extracapsular cataract removal with insertion of intraocular lens). In regions where Medicare has a higher physician payment for 0191T than for 66984, and where the payment for 66984 is reduced by 50%, payment for 66984-55 will be reduced by 50%.
| CyPass Micro-Stent | Hydrus Microstent | AqueSys | |
|---|---|---|---|
| Outflow Path | Suprachoroidal Space | Schlemm’s Canal | Subconjunctival Space |
| IOP Reduction | 35 to 40% at six months | Low 20s to mid-teens at six months | 6 to 8 mmHG at 12 months |
| Reduced Glaucoma Medications | Yes | Yes | Yes |
| Combined with Cataract Surgery | Yes | Yes | Yes |
Bottom line
Studies from the American Journal of Ophthalmology and the American Journal of Managed Care have shown that the majority of patients do not take their glaucoma medications as prescribed. Noncompliance is the No. 1 reason for drug therapy failure. Reducing the burden on medications not only benefits patients, it benefits the primary eyecare provider who will continue to manage the glaucoma for the rest of the patient’s life.
An implantation of a MIGS device provides confidence that IOP is being controlled around the clock and reduces the burden of medications. It is a win-win situation for the patient and the O.D.
With the steady rise in glaucoma patients, it’s critical to be prepared with the best possible treatment options. These patients will continue to explore options to treat their glaucoma safely and effectively. They will seek procedures to reduce the cost burden that is placed on them by medication usage.
MIGS achieve safety, are effective at lowering IOP and provide long-term cost savings to patients using multiple medications for glaucoma.
Further, MIGS can help eyecare providers on the front line of treating glaucoma by improving patient compliance and slowing the progression of the leading cause of irreversible vision loss. OM

| Dr. Schweitzer |