


CLINICAL
the front
CXL for Keratoconus and Ectasia
The link between you and patient success.
VISHAKHA THAKRAR, O.D., F.A.A.O., TORONTO, ONTARIO
Corneal collagen cross-linking (CXL) has dramatically improved the quality of life of many keratoconus and corneal ectasia patients.1,2 Specifically, the procedure addresses the condition’s underlying pathophysiology, as it can potentially delay and even halt corneal shape change.3 This, in turn, has enabled these patients to achieve improved vision and corneal topography and further reduce the likelihood of corneal transplantation.1-3
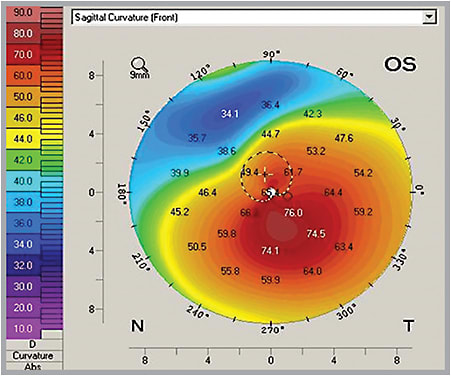
Shown is left corneal topography prior to CXL.
Although the procedure is currently under investigation in the United States, it likely won’t be long before it is FDA approved. As a result, it’s important you be prepared for your role in CXL for keratoconus and ectasia. Here, I define CXL and your forthcoming responsibility in patient care.
CXL defined
CXL involves the use of riboflavin (Vitamin B2) and UV-A radiation to improve corneal rigidity by increasing the biomechanical and biochemical stability of the stromal collagen fibers.4,5 Riboflavin functions to initiate cross-linking of the fibers when radiated with UV, while protecting the endothelium and other posterior structures from UV damage.1-9 By strengthening the collagen fibers, studies have shown improvements in corneal topography, higher-order aberrations and best-corrected and uncorrected visual acuity in keratoconic and ectatic patients.10-14
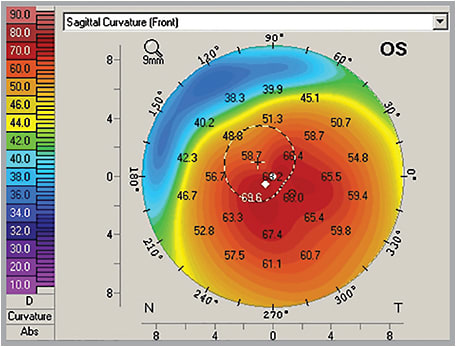
A little over two years post-CXL, the topography reveals flattening up to 7.00D to 8.00D in the same patient. Their BCVA with piggyback contact lenses was 20/70 prior to CXL and 20/25 at the 28-month mark.
The original Dresden Protocol, or standard procedure, involves removing the corneal epithelium, 7mm to 9mm in diameter, and applying riboflavin (0.1%) every one to five minutes for 30 minutes.1,3 Then, the eye is exposed to UV-A (370nm) and a surface irradiance of 3mW/cm2 for 30 minutes.2
Corneal thickness should be maintained at 400 u throughout the procedure after the epithelium is removed to prevent endothelial cell loss.1,4,15 It has been more recently demonstrated that if the cornea is thin (between 330 u and 400 u), hypotonic solution can be applied to artificially swell the cornea to 400 u.4,15,16 But, this is considered too risky if the cornea is thinner than 330 u.4,15,16
Finally, bandage contact lenses are applied for approximately five days to promote re-epithelialization and reduce pain.
Although still considered investigational, accelerated CXL is being used in surgical centers throughout the United States.17 This procedure involves increasing the irradiance of UV-A while decreasing the exposure time to maintain the same overall energy level as the standard procedure.16 The results have been promising, although long-term investigations are necessary to determine whether the accelerated approach will be as safe and effective as traditional CXL.16,17,18 A modification of this procedure, called pulsed accelerated CXL, involves using pulsed rather than continuous UV-A in an oxygen-rich environment. This procedure has the potential to provide increased stiffening.17
MORE ON THE “ANTERIOR”:
JULY 2013
Anterior Segment in Review • page 14
OCTOBER 2012
Update on Femtosecond Technology • page 41
JUNE 2012
CXL: Strengthening the Ties That Bind • page 48
CXL can also be conducted in combination with PRK (Athen’s Protocol) and with intracorneal ring segments (ICRS) implantation. The goal of Athen’s Protocol is to improve vision by normalizing the cornea.19 This procedure involves removing the epithelium with PTK and using topography-guided partial PRK to steepen the flatter area adjacent to the cone while correcting some of the irregular astigmatism.19 Maximum treatment of the corneal stroma should not exceed 50 u.19 The cornea is then immediately cross-linked. The procedure is believed to yield better visual results than performing PRK and CXL separately.20
Similarly, the goal of the ICRS implantation is to flatten and regularize the cornea while halting the progression with CXL.21 It has been suggested the ICRS be implanted first, followed by CXL on the same day for optimal results.22
Many other CXL variations are currently under investigation. In fact, an article in the September 2013 issue of the Oman Journal of Ophthalmology, by Messmer, and an article in the January 2012 issue of the American Journal of Ophthalmology, by Hovakimyan and colleagues, discuss current and future CXL modifications.23,24
Patient selection
Patients who have progressive keratoconus or ectasia and are between the ages of 9 and 35 may be candidates for CXL.25,26 The reason: As patients age, the cornea tends to cross-link itself, which results in reduced progression of the disease.25,26,27 Research has shown that the effect of cross-linking is less pronounced in patients older than age 40, although this group still showed improvements in refractive, topographic and aberrometric results.27 Also, research suggests that, ideally, corneas less than 58.00D should be treated, although corneas steeper than this can be treated at the surgeon’s discretion.15 There is, however, an increased chance of sight-threatening corneal haze in advanced keratoconus.15 In cases in which corneal progression is questionable, topographies taken six months to one year apart may detect differences.
Contraindications to CXL are dense, central corneal scarring, autoimmune disease, history of herpes keratitis, very thin corneas and severe dry eye.15,23
Patient education
As successful post-operative outcomes hinge, in part, on patient expectations, managing these expectations prior to the surgery is crucial. As a result, patients should be educated that they may initially experience blurred vision, ocular discomfort and photophobia post-operatively. Also, inform patients of the complications — reported 2.9% to 3.5% — which are loss of BCVA, dry eye, corneal melt, corneal haze, endothelial cell loss, infectious keratitis and reactivation of herpes keratitis.3,26,28
Explain to your contact lens-wearing patients that they will likely be able to restart lens-wear two to four weeks after surgery, though their cornea can continue to change throughout the next few years, resulting in the need for new contact lenses.27
Post-op management
An optimum post-CXL outcome also depends on post-operative management. Typical post-op management includes fluoroquinolones, topical steroids and artificial tears. The dosing and amount of time used is relative to the surgery center. For example, a topical fourth generation fluoroquinolone q.i.d. for seven days, a topical corticosteroid q2h for two days, q.i.d. for five days, and then tapered through the next six to seven weeks. Also, non-preserved artificial tears q2h for the first two days, and as needed thereafter. I typically recommend artificial tears at least q.i.d. for the first month. Patient post-operative visits can include: Day one, Day three through five, Day ten, Month one, Month three, Month six and one year. The bandage contact lenses are commonly removed after roughly five days, as this is usually when the epithelium is intact.
Patients can wear glasses or soft contact lenses post-operatively in mild cases of keratoconus and specialty soft, gas permeable, hybrid or scleral lenses in moderate to severe cases. Unfortunately, fitting a post-CXL cornea is essentially fitting a fluctuating cornea. Typically, the cornea steepens, and can flatten for up to several years afterwards.
When dealing with an established contact lens wearer, I try to defer the contact lens refit as long as the patient’s vision and fit are acceptable in their current lens, and corneal integrity isn’t compromised.
When post-CXL patients require a new contact lens fit, I try to avoid fitting these eyes until at least two to four months postoperatively, since the cornea shape is fluctuating during that period. In addition, I encourage many of them to wear scleral lenses because these lenses completely vault the cornea and therefore, can be more forgiving to corneal changes. Nevertheless, the cornea is still changing, most likely flattening, which may result in a steep fit through time. (However, scleral lenses that are too steep can cause limbal bearing and reduce oxygen to the cornea due to increased thickness of the post-lens tear layer.29 These issues should be addressed by refitting the lens.) After the fit is complete, I continue to monitor post-CXL contact lens patients every three months in the first year and every six months thereafter until I feel sequential corneal topographies are stable.
Doing our part
Not long ago, managing keratoconus was limited to glasses and contact lenses. Data from multiple CXL studies reveal the tides are turning. So, prepare for comanagement. OM
References are available in the online version of this article at optometricmanagement.com.

| Dr. Thakrar has a specialty contact lens practice outside of Toronto, Ontario and is a clinical optometrist at TLC Laser Eye Center. E-mail her at thakrarv@gmail.com, or send comments to optometricmanagement@gmail.com. |