


CLINICAL
the front
Managing Severe Herpes Keratitis
The goal is to decrease frequency and do our best in preserving the eye’s normal appearance and function
J. JAMES THIMONS, O.D, F.A.A.O., FAIRFIELD, CONN.
Few, if any, diagnoses are more challenging and potentially sight-threatening than severe herpes keratitis. After all, once the classic dendritiform herpetic presentation evolves into disciform, iritic, limbal and geographic disease, clinicians are faced with a disease process that adds layers of complexity in management and can produce vision loss through the therapy course, along with other co-morbid complications, such as cataract and, occasionally, the need for enucleation.
Severe herpes keratitis is especially common in the elderly, or those who have a compromised immune status. Thus, the goal for these patients is to decrease the relative rate of recurrence and maintain the most normal anatomic and physiologic status of the eye.
Here, I discuss how I’ve managed such a patient for the last decade.
Stromal disciform herpes
Roughly 10 years ago, J.R., a man in his late 70s, presented with stromal disciform herpes in his right eye. Visual acuity OD was in the 20/300 range, with pinhole, and the eye had a low-grade iritis, along with overlying pseudo-dendritiform lesions of the cornea.
I prescribed prednisolone acetate ophthalmic suspension to quiet the inflammation and 500mg of valacyclovir hydrochloride (Valtrex, Glaxo Smith Kline) for prophylaxis against viral reactivation.
The episode resolved after approximately six weeks, although a notable cataract was now present (not uncommon in these cases). J.R.’s vision at this visit was 20/150 OD. I prescribed a maintenance dose of oral acyclovir, and I suggested that we delay cataract surgery due to the recent disease activity of the stromal region.
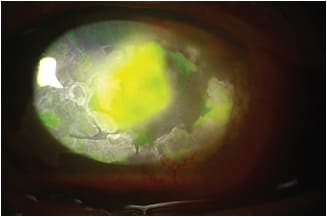
The patient had advanced herpetic keratitis with a microbial superinfection.
Recrudesced disciform and iritic episodes
Through the years, J.R.’s disciform lesion returned along with iritic episodes — both of a relatively severe nature despite acyclovir use.
At each event, the corneal architecture further eroded, inducing corneal thinning and visual distortion from scarring, both of which, along with the cataract, caused his VA to decline to FC@3ft/ Ph 20/400.
Through the course of treatment, I noted intermittent IOP elevations. Also, the cataract continued developing, playing an increasing role in the patient’s vision change, so I referred J.R. for a surgical consult. Citing the level of herpetic activity in that eye, the surgeon decided to delay intervention.
During this time, the patient’s IOP began spiking into the high 20s, and a keratouveitic glaucoma developed, which I managed with topical anti-ocular hypertensives b.i.d., topical steroids and low-dose oral acyclovir on a continued basis between recrudescence episodes.
Intense band keratopathy
As the disease progressed and J.R.’s vision remained reduced, the cornea began to develop excessive band keratopathy, which eventually navigated the entire palpebral aperture. The band keratopathy became quite rigid and periodically fractured, resulting in patient complaints of foreign body sensation. I considered using ethylenediaminetetraacetic acid and scraping the cornea, but I decided against it because neither would aid the patient’s visual function, and the occasional foreign body sensation was a small concern relative to possibly reactivating the virus with these treatments. Instead, I debrided the band keratopathy when symptomatic and used a short-term bandage contact lens for comfort.
After a relatively stable period, J.R. presented with an area of band keratopathy, which extruded itself and subsequently opened the central cornea. The band keratopathy that detached was approximately 2.5mm to 3mm and resulted in a sub-300µ thickness over a notable portion of the central cornea. Exam revealed no evidence of corneal staining or other damage to the underlying epithelial surface, so I prescribed a topical fourth-generation fluoroquinolone q.i.d. and preservative-free lubricant eye ointment q.i.d. (to be used 10 minutes after the fluoroquinolone) for a one-week period and scheduled the patient for a follow-up visit.
Eye ache, nausea, dizziness
Before the next appointment, J.R. called my practice complaining of a foreign body sensation and, more importantly, an ache within the eye, nausea and a sense of equilibrium loss.
On presentation, the original area from where the band keratopathy spontaneously extruded had now developed a 5mm to 6mm central corneal ulcer, with significant necrosis at its margin. Also, a 1/4-level hypopyon was present in the anterior chamber. (Of note: Patients who have herpetic disease are susceptible to bacterial over-infection secondary to the neurotrophia and localized decrease in immune status.)
I cultured the eye on blood, chocolate, thioglycolate and Sabouraud’s agar. While awaiting results, I prescribed a fortified antibiotic 25mg/ml and a topical fourth-generation fluoroquinolone alternating Q 1 hour. Additionally, I added topical bacitracin zinc-neomycin sulfate-polymixin B Sulfate (Neosporin, Johnson & Johnson) as a supplement until the fortified antibiotic, which had to be compounded, was available.
After a two-day course of this treatment regimen, J.R. showed a reasonable response, so I prescribed an anticholinergic medication q.i.d. to alleviate the discomfort. There was an improvement in symptoms without VA change.
Biologic corneal bandage
On the seventh post-treatment day, though the patient said he felt better, the ulcer was beginning to considerably thin, and J.R. was down less than 200µ of central corneal thickness. This obviously created a concern relative to corneal perforation and the potential for endophthalmitis and possible enucleation. Since the cultures had come back positive for MRSA with a slight presence of gram-negative Pseudomonas aeruginosa, the prescribed drugs were sensitive to these organisms. So, I decided to add a biologic corneal bandage to assist in corneal repair.
J.R. maintained all medical therapy during use of the biologic corneal bandage, and five days after its placement, the margins of the ulcer decreased 60% to 70%. The cornea had stabilized, the anterior chamber had quieted appreciably, and he said the nausea and dizziness abated. As a result of the success of the first biologic corneal bandage, I placed a second one, and the patient subsequently stabilized completely after another week of treatment.
Even though this episode resulted in a reasonable outcome, J.R. was at an increased risk for a “herpetic melt” and loss of the globe. As a result, I discussed the need for a conjunctival flap, which would effectively stabilize the cornea and therefore, relatively eliminate the risk of melt with perforation in the future. The patient agreed to undergo this procedure once the eye completely quieted.
Interestingly, during this period, J.R.’s IOP dropped dramatically, and I ceased topical therapy. This is most likely secondary to damage to the ciliary body and the beginnings of phthisis, which will eventually make the eye non-functional.
Current status
J.R. has resolved the “superinfection” of the herpetic lesion, and he says his eye is comfortable. The conjunctival flap is scheduled in the next few weeks, and it is anticipated that it will stabilize the eye long-term. Sadly the damage done by the disease has been at the expense of sight and cosmetic status, yielding a very “ugly cornea” as a consequence. OM

| Dr. Thimons practices in Fairfield, Conn. and is adjunct clinical professor at the New England College of Optometry and the Pennsylvania College of Optometry at Salus University. He is also chairman of the National Glaucoma Society. E-mail him at jthimons@sbcglobal.net or send comments to optometricmanagement@gmail.com. |