


CLINICAL
POSTERIOR
WHAT CAUSED THIS DETACHMENT?
WAS THE CULPRIT A RETINAL TEAR, TRAUMA OR BOTH?
SHERROL A. REYNOLDS, O.D., F.A.A.O.
A 65-YEAR-OLD Hispanic male presented complaining of decreased vision OS for one week. The patient said it started after a minor fender bender that occurred around the same time. He denied sustaining any head trauma or needing medical care. The patient also reported symptoms of floaters, described as multiple fine dots, and flashes of light that were worse in dimly lit rooms OS. He said these symptoms started a month ago, but had increased in intensity and frequency since the car accident. His medical history is significant for hypertension and atherosclerosis for which he takes medication.
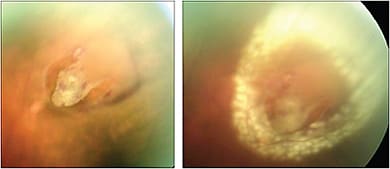
The patient’s BCVA was 20/20 OD and 20/200 OS, with no improvement on pinhole testing OS. Examination revealed a relative afferent pupillary defect OS. Ocular motilities were unremarkable, but confrontation visual field OS revealed peripheral temporal field loss. Dilated exam showed normal findings OD. In OS, pigmented cells, tobacco dust, or Shafer’s sign, was noted in the vitreous. Retinal exam revealed a retinal detachment (RD) with the macula off and a peripheral horseshoe (flap), or u-shaped, retinal tear in the superior retina with surrounding subretinal fluid.

About 50% of patients with symptomatic horseshoe tears will develop RD, according to the journal “Ophthalmology.”
Did the retinal tear, car accident trauma or both cause this patient’s RD?
Here, I discuss the etiology, symptoms, clinical signs and management options for retinal breaks and the cause of this patient’s RD.
ETIOLOGY
A break in the retina, defined as a full-thickness retinal defect, is categorized as a tear or a hole. Most retinal breaks are caused by vitreous traction at the vitreous base, a site of strong vitreoretinal adhesion, during a posterior vitreous detachment (PVD). In fact, about 26% of patients with acute PVD will have a concomitant retinal tear at the initial presentation, according to the “American Journal of Ophthalmology.” Even after the initial examination, these patients have a 2% to 5% risk of developing a retinal tear in the weeks that follow.
Other risks for retinal breaks are vitreoretinal traction at the margin of lattice degeneration, which runs parallel to the ora serrata (while lattice degeneration occurs in 5% of eyes, especially in moderate to high myopes, it is found in 30% of all eyes with RD, according to “Ophthalmology”), advancing age, cystic and zonular tractional tuff, history of prior retinal breaks or RD, prior retinal surgery, blunt or penetrating trauma, moderate to high myopia and a family history of retinal breaks and/or RD. Retinal breaks do not discriminate in terms of sex.
Retinal breaks can be classified into three categories: (1) atrophic holes, (2) operculated holes and (3) horseshoe tears.
Atrophic holes are the most common types and are not associated with vitreoretinal traction. They are the result of atrophic changes within the sensory retina and occur frequently within areas of lattice degeneration. Operculated holes are the result of avulsion, or relief, of vitreoretinal traction from the retinal surface, resulting in the operculum. Neither type of break is likely to cause a RD.
Horseshoe tears are the most ominous retinal breaks and result from persistent vitreoretinal traction during a PVD. Because of the persistent traction, these tears have a higher risk of causing a RD. In fact, about 50% of patients with symptomatic horseshoe tears will develop a RD, according to “Ophthalmology.” Further, approximately 5% of eyes with asymptomatic horseshoe tears progress to RD, according to the “British Journal of Ophthalmology.”
SYMPTOMS
While some retinal break patients are asymptomatic, it is important to be aware of symptoms that are red flags for retinal breaks.
• New onset floaters, described as cobwebs, veils, bugs, a ring and single or multiple spots.
• New onset of flashes, either bright light or streaks similar to a lightening streak.
Patients who experience symptoms of flashes of light and floaters during an acute PVD have an increased risk of developing a retinal tear that leads to a RD.
• Photopsia (from vitreoretinal traction)
• VA: normal with retinal breaks, but decreased if retinal breaks lead to a RD with macular involvement.
• Peripheral visual field defects, described as a “black curtain” or “shadow” (indicative of RD)
• An afferent pupillary defect (chronic RD)
CLINICAL SIGNS
Each of the aforementioned categories of retinal breaks have their own clinical signs:
1. Atrophic holes. These are round retinal holes that range from a pinpoint to about a two-disc diameter, with or without surrounding pigment, which represents chronicity of the hole. They are observed as an isolated finding or with lattice degeneration. They are often asymptomatic and have a very low risk for progression to RD.
2. Operculated holes. These are round, red holes with an overlying free-floating plug, or operculum, attached to the vitreous. As with atrophic holes, they can develop a pigmentary demarcation line, are often asymptomatic and rarely lead to RD, unless vitreoretinal traction persists in the vicinity of the hole.
3. Horseshoe. This consists of a flap or sensory retina where its apex is pulled anteriorly by the vitreous while the base remains attached to the retina. Horseshoe tears are more common in the superior temporal quadrant followed by the superior nasal quadrant.
Ominous clinical signs of horseshoe tears are pigment cells in the vitreous (tobacco dust or Shafer’s sign), suggestive for a retinal tear in 70% of cases, according to “Ophthalmology,” red blood cells observed in the anterior vitreous, suggesting the presence of multiple breaks or superior location of break, a “cuff” of subretinal fluid surrounding the retinal break or the presence of vitreous hemorrhage with a PVD.
Up to 80% of patients who presented without detected breaks, and then had breaks occur subsequently, had either pigmented cells or hemorrhages in the vitreous or retina at the initial evaluation or symptoms that prompted a return visit, according to the “American Journal of Ophthalmology.”
DIAGNOSIS/MANAGEMENT
To diagnose a retinal break or RD, employ the following:
• Slit lamp. This will enable you to look for pigment cells, red blood cells and/or vitreous hemorrhage.
• Condensing lenses. Those with a large field of view will help you identify peripheral changes and retinal breaks.
• Fundus photography. Widefield retinal imaging offers panoramic fundus assessment that can help you to detect the presence of a retinal tear or RD.
• SD-OCT. This helps identify the presence of PVD-associated changes, such as vitreomacular adhesion/traction as the underlying cause of the patient’s complaint and aids you in ascertaining the status of the macula.
• B-scan ultrasound. This is beneficial in detecting the retinal break or RD if there is media opacity (vitreous hemorrhage or significant cataract).
In terms of management, asymptomatic atrophic and operculated retinal holes rarely lead to RD, due to the lack of traction. Therefore, thoroughly educate these patients on the symptoms of flashes of light and floaters; and monitor them for change on yearly visits. The American Academy of Ophthalmology’s Preferred Practice guidelines recommend that patients with symptomatic PVD sans retinal breaks be monitored initially every one to eight weeks, depending on the patient’s risk factors for a retinal tear and clinical findings, like pigment in the vitreous. Vitreomacular traction should also be considered as a cause of the patient’s symptomatic PVD. After initially being monitored closely, these patients should be followed up with every three to six months.
Up to 16% of patients who have a retinal tear will develop additional breaks during long-term follow-up.
PHOTO COURTESY: Illinois & Retina Eye Associates
Symptomatic horseshoe tears should be referred to a retinal specialist for prompt treatment in the form of a laser burn or cryotherapy around the hole or tear to create a complete, firm chorioretinal adhesion to prevent RD. Half of untreated symptomatic retinal tears will lead to RD, while with treatment the risk of RD occurring is approximately 5%, according to the “British Journal of Ophthalmology.” Moreover, patients with asymptomatic horseshoe tears should be monitored every three to six months because of a small risk of RD.
During follow-up care, it is important to assess treated tears for a well-sealed barrier, as continued traction may lead to RD. Be sure to study the peripheral retina for the presence of new breaks as well. Up to 16% of patients will develop additional breaks during long-term follow-up, according to the “American Journal of Ophthalmology.” Carefully assess the patient’s other eye, as there is a 10% increased risk of developing RD in the fellow eye says “Ophthalmology.”
THE ANSWER
If you think the patient’s RD was due to both the tear and the trauma from the car accident, you are correct! The superior horseshoe tear predisposed the patient for the development of an RD, but the risk increased from the trauma of the car accident. This patient was immediately referred to a retinal specialist for surgery. There was modest improvement in his vision to 20/60 OS post surgery. The patient is now closely monitored with three-month follow-up care.
Retinal breaks, mainly retinal tears, especially those associated with a PVD can pose a serious threat to vision with the potential development of a RD. Patients with risk factors need to be thoroughly educated on their condition and monitored closely, while those in danger of a RD require urgent consultation. OM

| DR. REYNOLDS is an associate professor at the Nova Southeastern University College of Optometry and clinical preceptor/attending in the college’s diabetes and macular clinic. She is a fellow of the Optometric Retina Society and chairperson for the Florida Optometric Association Healthy Eyes Healthy People Committee. Comment at tinyurl.com/OMcomment. |