


CLINICAL
pediatrics
Pediatric Eye Disease Awareness
Rare will eventually land in your chair
LEONARD J. PRESS, O.D., F.A.A.O., F.C.O.V.D.

The Pediatric Eye Disease Investigator Group (PEDIG) includes a list of published studies on various topics, such as amblyopia, strabismus, stereopsis and hyperopia — clearly not the problems one thinks of when referring to pediatric eye disease.
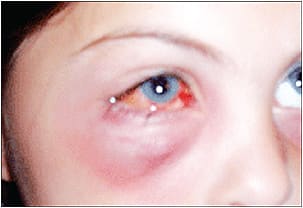
Note the acute eyelid erythema and edema in this preseptal cellulitis patient.
My point: As unlikely as it is that the children you see who have amblyopia or strabismus will have active disease processes, it is nevertheless important to consider the possibility that, at some point, a rare case might end up in your chair, and missing it could have dire consequences. (Retinoblastoma and cortical visual impairment in infants are prime examples.)
Here, I discuss other ocular problems, the tools needed for diagnosis and how you should manage them.
Ocular problems
In addition to retinoblastoma and cortical visual impairment, optometrists should be aware of these four types of eye problems in children:
1 Nasolacrimal duct obstruction. This is a common disease of infancy, occurring in approximately 5% of all infants. In about 90% of these cases, the condition resolves spontaneously, whereas 10% of cases require treatment of some sort. Treatment is conservative at first, consisting of tear duct massage before more aggressive measures of tear duct probing or balloon tear duct dilation.
2 Preseptal cellulitis. This pediatric eye disease occurs more commonly, particularly among young children, in whom the eye or eyes begin to look “nasty” (acute eyelid erythema and edema) very quickly. Differential diagnosis and timely interventions through referral are often necessary, particularly for hospital admission and treatment with IV antibiotics.
Preseptal cellulitis may be mistaken for orbital cellulitis, which may have the same signs and symptoms in the periorbital tissue but also result in proptosis as a result of more posterior involvement.
3 Systemic disease-caused eye problems. It is important to be aware that certain pediatric eye diseases are associated with systemic diseases.
For example, childhood glaucoma is linked with juvenile diabetes. In addition, children may present with early neuro-ophthalmic signs of multiple sclerosis, such as oscillopsia and diplopia.
By learning about the congenital syndromes involving the extra ocular muscles, you’ll be better able to differentiate infantile from acquired conditions and, perhaps, play a role in the diagnosis of the systemic condition. I recommend Genetic Diseases of the Eye (Oxford University Press; 2 edition (December 29, 2011).
4 Sports-induced eye problems. Children participating at younger ages in a variety of sports are prone to head injuries, which can cause eye problems, such as blurred vision and photophobia. In fact, football, hockey and soccer are the main culprits.
Keep abreast of how eyecare practitioners are playing an important role in diagnosing and treating ophthalmic signs of concussion in children, so you can follow suit. (See “The How and Why of mTBI” at http://bit.ly/1HAa7QV.)
Needed tools
In order to diagnose pediatric eye disease, you’ll need one tool in particular: a slit lamp. Although use of the conventional slit lamp is ideal for older children, young children may require use of a handheld slit lamp because they tend to have trouble sitting still and may be too small to reach the conventional slit lamp. An array of portable models are available, including those with iPhone adapters.
Something else to consider: Don’t hesitate to try automated fields on young children. That said, have confrontation fields with attractive lights or finger puppets as a backup plan.
Management
The challenge in managing any of the four pediatric eye diseases is to strike a balance between appropriate reassurance and being an alarmist. For example, when a child develops a tic that results in rapid spasmodic blinking, reassurance is all that is needed. If stress is an underlying factor, the use of artificial tears might be justified as a placebo of sorts.
On the other hand, children who have persistent tics can show signs of dry eye disease or various forms of conjunctivitis, for which appropriate topical agents are important.
Be ready
When seeing children in your practice, pediatric eye disease comes with the territory. Knowing how to recognize and manage these conditions gives parents confidence in your skill set. OM
DR. PRESS IS THE OPTOMETRIC DIRECTOR OF THE VISION & LEARNING CENTER IN FAIR LAWN, N.J. HE SPECIALIZES IN PEDIATRIC VISION. HE COMPLETED HIS RESIDENCY PROGRAM IN PEDIATRIC OPTOMETRY AT THE EYE INSTITUTE OF THE PENNSYLVANIA COLLEGE OF OPTOMETRY, AND HE SERVED AS CHIEF OF THE PEDIATRIC UNIT OF THE EYE INSTITUTE. IN ADDITION, HE’S A DIPLOMATE OF THE AAO AND HAS WRITTEN THREE TEXTBOOKS ENCOMPASSING PEDIATRIC OPTOMETRY AND IS A DIPLOMATE IN THE PEDIATRIC OPTOMETRY/BINOCULAR VISION AND PERCEPTION SECTION OF THE AAO. E-MAIL HIM AT VISIONLECTURE@GMAIL.COM, OR SEND COMMENTS TO OPTOMETRICMANAGEMENT@GMAIL.COM.