


MEDICAL SERVICES
medical necessity
Medically Necessary Contact Lenses
Why and how to incorporate these lenses into your practice
MELISSA BARNETT, O.D., F.A.A.O., F.S.L.S., SACRAMENTO, CALIF.
Creating a specialty contact lens practice can be extremely rewarding, as you’re providing optimal vision correction to the most challenging cases, while boosting practice revenue.
Here, I define medically necessary contact lenses (MNCLs), the protocol for fitting, insurance coverage and the latest codes to facilitate offering this service in your practice.
MNCLs defined
MNCLs help improve visual acuity, reduce or eliminate visual aberrations and enable patients to function in everyday life in a way that spectacles and conventional contact lenses cannot. They also improve peripheral vision and reduce asthenopia and glare.
There are many conditions that are considered medically necessary, including corneal ectasias (e.g., keratoconus, keratoglobus or pellucid marginal degeneration) and post-surgical ectasia (e.g., post-LASIK, post-PRK or post-corneal transplant). Aphakia, aniridia, severe dry eye caused by Sjögren’s syndrome, graft-versus-host disease or Stevens Johnson Syndrome are other examples.
Keep in mind, each visioncare and medical plan has its own standard contractual definition of medical necessity as it applies to contact lenses.
Protocol for fitting
Here is how I incorporate MNCLs into my practice.
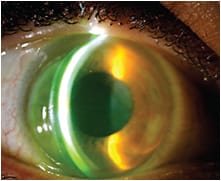
A scleral lens was used to correct irregular astigmatism, providing good vision. In addition, the patient’s dry eye improved and sensitivity to light was eliminated.
1. Determine the patient’s needs. The patient must have reduced vision that cannot be corrected by conventional glasses or standard contact lenses. When evaluating a patient for MNCLs, the chief compliant must logically correspond to the covered service, which must be documented and ordered. In addition, testing performed should have a specific indication. It should not be done just because “you have a covered diagnosis.” The test results must influence the treatment plan. For example, a topography should be performed in order to provide information for a fitting.
Likewise, contact lens treatment should be the standard of care. In other words, a treatment cannot be for convenience, such as cosmetic.
2. Schedule the appointment. When scheduling an appointment, the patient is identified with a medically necessary condition and then scheduled for a specific appointment for MNCLs. Our authorization coordinator obtains a prior authorization from the patient’s insurance provider for the fitting (technical component) and materials, and the patient is informed of the coverage.
It is invaluable to confirm eligibility beforehand, not only to save time, but it allows you to fit the patient with MNCLs at the time of the appointment instead of having to wait hours, days or weeks for authorization.
3. Prepare the patient. Provide an educational brochure that explains the process of prescribing MNCLs so the patient knows what to expect.
4. Discuss and sign the necessary forms. When the patient arrives, we have him sign a contact lens waiver. This form outlines our policy regarding the contact lens prescription, reviews why a contact lens evaluation or fit is necessary and the range of fees involved. It also reviews necessary follow-up appointments and makes the patient aware of exactly what the MNCL fee does and does not cover, including contact lens exchanges and office visits.
If the patient has Medicare, he signs an advance beneficiary notice of non-coverage (ABN), which is required for Medicare and is accepted by other carriers. The ABN is the best method to inform patients of suspected out-of-pocket costs and that they may be responsible for payment should their carrier deny the claim.
The practitioner must state the likely reason that the claim may be denied and that the ABN is not a blanket form to be used arbitrarily. The ABN form gives three options: (1) the service is provided and insurance is billed; (2) the patient is responsible for payment and insurance is not billed; and (3) service is declined. The patient chooses one of these options and signs the form. The ABN is not submitted to the carrier, but the specific service provided that is related to the ABN has a modifier appended to it that best describes the action surrounding the ABN, such as GA, GX, GY, & GZ. (For more information on modifiers, visit cms.gov.)
4. Perform the necessary tests. My technician starts the examination with testing, including visual acuity and corneal topography or anterior segment tomography.
5. Discuss options; fit the patient. I discuss MNCL options and fit the patient with the most appropriate type of contact lens. During fitting, I reiterate to the patient that the fitting is a process and may take multiple visits to complete. Staff can help by reviewing the fitting process, expected follow-up visits and appropriate fees depending on the patient’s medical condition and contact lens requirements.
6. Complete billing forms. A billing form is filled out and sent to our billing department. MNCLs are ordered.
7. Schedule follow-up visit. Before the patient leaves, additional appointments are arranged for any follow-up visits.
Insurance coverage
Both medical and visioncare plans may cover services and/or materials associated with MNCLs. Each plan has its own definition and list of covered diagnoses. In general, Medicare does not cover MNCLs.
In some instances, a coordination of benefits may be indicated. For example, if a visioncare plan does not cover pachymetry and topography, it may be necessary to bill the patient’s medical insurance. Keep in mind that you must follow your separate contract with the medical carrier with respect to deductibles and/or copays.
Some third party payers additionally offer full coverage of spectacle lenses (not frames) to wear over MNCLs. It is important to read each third party payer’s individual policy, as the policy may change at any time.
Latest codes
Since Jan. 1, 2012, there has been a change in the CPT codes for therapeutic contact lenses. CPT Code 92070 became obsolete and was replaced with codes 92071 and 92072.
• 92071: Fitting of a contact lens for the treatment of ocular surface disease. Note this code is only for fitting, and materials should be billed separately, using either 99070 or the appropriate HCPCS Level II material code. This is a unilateral code.
• 92072: Fitting of a contact lens for management of keratoconus, initial fitting only. Note this code is only for fitting, and materials should be billed separately, using either 99070 or the appropriate HCPCS Level II material code. This was originally a unilateral code, but in mid-2012 the CMS and AMA changed this code from unilateral to bilateral.
Each carrier’s plan will vary in payment for these codes. It is helpful to read each contract in advance to determine what the contract specifies for each code used. It is important to use the correct codes and modifiers for each medically necessary contact lens fit. Most importantly, it is pertinent to bill appropriately for all services.
When needed, send letters of medical necessity to insurance plans. It may be helpful to create a modifiable letter template that explains why contact lenses are a medical necessity.
MNCL success
Specialty contact lenses can change patients’ lives for the better, leading to more satisfied patients and a healthier bottom line for you. OM

| Dr. Barnett is a principal optometrist at the UC Davis Medical Center in Sacramento. She has worked with Acculens, Alcon, Alden Optical, Allergan, CooperVision, Nidek and Vistakon. Send comments online to tinyurl.com/OMcomment. |