


CLINICAL
POSTERIOR
BANISH BRAO
A PRIMER ON HOW TO DIAGNOSE AND MANAGE THIS CONDITION
BRANCH RETINAL artery occlusion (BRAO) represents approximately 38% of all acute retinal artery obstructions, according to Archives of Ophthalmology. BRAO frequently occurs due to an embolic obstruction, leading to retinal ischemia in the affected area. It has the potential to permanently impact vision and, more importantly, can indicate a serious underlying systemic disease, such as carotid artery disease, which can lead to a stroke and early death. As such, identification and proper management of BRAO can not only save your patients’ vision, but perhaps save their lives.
Here, I discuss the etiology, symptoms, clinical signs and what you, as a primary eyecare provider, can do to manage this condition.
ETIOLOGY
Risk factors for BRAO include the following:
• Age >60 (If BRAO occurs in patients younger than 40, the possibility of blood-clotting disorders, congenital heart disease or oral contraceptive use must be investigated.)
• Gender (Men are more commonly affected than women.)
• Carotid artery disease
◦ Atheromatous plaque
• Hypertension
• Dyslipidemia
• Diabetes
• Smoking
• Cardiac disease and lesions (i.e., Mitral valve lesions and bacterial endocarditis)
• Inflammatory or rheumatological diseases (i.e., GCA-giant cell arteritis)
• Coagulopathies
◦ Sickle cell disease
◦ Hodgkin’s disease
◦ Pregnancy
◦ Anemia
• Platelet and clotting factor abnormalities (i.e., homocystin-uria, Protein C and S deficiencies, and antiphospholipid syndrome)
• Certain medications (oral contraceptives, erectile dysfunction and hormone medications)
Back to Basics: Ocular Massage
To attempt ocular massage, have the patient close his or her eye, then massage and apply pressure for 10 to 15 seconds. This may produce retinal arterial dilation, with the hope of improving perfusion or dislodging the obstructing emboli or thrombosis. Check the retina after each attempt.
The main cause of BRAO is an embolus that has traveled through the bloodstream, becoming trapped in the smaller-caliber retinal arteries. Emboli are frequently found in patients with the aforementioned systemic conditions. There are three types of emboli, with cholesterol being the most common, followed by calcific and platelet-fibrin. Other less common types include emboli from tumors, migraines, parasitic or fungal injections, Susac syndrome or impurities injected into the bloodstream from intravenous drug use. Non-embolic causes, such as thrombosis and atherosclerosis, also play a role in the pathophysiology of BRAO.
SYMPTOMS
BRAO symptoms include acute, painless, unilateral partial vision loss. Vision loss can vary from mild to severe (finger counting or hand motion), depending on the location of the involved retina. Patients often do not notice any changes to their vision with non-macular BRAO. The visual prognosis tends to worsen with macular involvement and BRAO duration.
CLINICAL SIGNS
Retinal findings:
• Narrowed branch retinal artery
• A wedge-shaped area of superficial retinal whitening in the affected retina (commonly in the temporal arcade)
• Boxcarring, segmentation of blood flow in the retinal vessels
• Emboli, which are visible in 62% of eyes with a BRAO, according to the Annals of Ophthalmology, and are frequently seen at a bifurcation where they characteristically lodge due to a narrowed lumen
◦ Cholesterol emboli (also known as Hollenhorst plaques, yellowish plaque indicating carotid artery disease)
◦ Platelet-fibrin emboli (whitish-gray, non-reflective plaque indicating thrombotic disease)
◦ Calcific emboli (large, yellowish-white plaques indicating cardiac disease)
• Sclerosed arteriole
• Collateral vessels (rare); artery-to-artery collaterals may form in the retina and are highly suggestive of an old branch retinal artery obstruction.
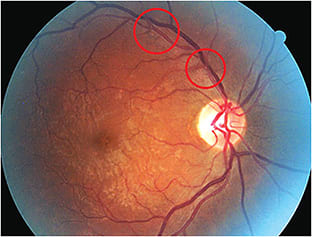
HF, a 58-year-old female with a BCVA of 20/20 OD and 20/20 OS, had a medical history of hypertension and hypercholesterolemia. Ocular exam revealed multiple areas of cholesterol emboli OD that could lead to a BRAO. Further testing revealed carotid artery disease and the patient was treated.
A careful history aimed at identifying previous neurological episodes of amaurosis fugax, transient ischemic attacks or cerebrovascular accidents (strokes) should be taken in all suspected BRAO patients. According to Retina, amaurosis fugax occurred in 14.2% of BRAO patients. O.D.s should also inquire about other potential causes of emboli, such as blood clots, which may lead to an increase risk of recurrent BRAO.
Contingent on the size of the BRAO, pupil examination may reveal an afferent pupillary defect. BRAO patients may have visual field defects that correspond to the occlusion site. Presenting field defects may include a central scotoma, a superior or inferior altitudinal defect. Serial visual field testing is recommended to monitor stability or improvement of field deficits.
BRAO occurs at an arteriovenous bifurcation, more commonly in the superior temporal retina. The initial area of retinal whitening dissipates through time as the edema resolves and the retina coloration returns to normal. A sclerosed ateriole may result from lack of perfusion and can be the only remaining visible evidence of previous occlusion.
Visual prognosis after a BRAO, when compared with its counterpart, central retinal vein occlusion, is often favorable. Eyes with an initial visual acuity of 20/40 or better usually remain at 20/40 or better. Individuals with poor visual acuity, such as 20/100 or worse, generally do not show any significant improvement.
MANAGEMENT
A detailed medical work-up, including a cardiology evaluation with an echocardiogram, is the most important management of all BRAO patients. According to Archives of Clinical and Experimental Ophthalmology, patients with both the presence of a visible retinal embolus and a BRAO have a worsened survival prognosis. Particular attention should be directed at the presence of hypertension; therefore, blood pressure and pulse should be evaluated at baseline and at follow-up evaluations. Carotid artery palpation and auscultation can be easily performed during a baseline examination in all BRAO patients. Diabetes screening, clotting factors, erythrocyte sedimentation rate or C-reactive protein screening, especially in patients older than 50, should be ordered. Blood cultures to evaluate for bacterial endocarditis and septic emboli, as well as a carotid artery and cardiac evaluation with echocardiography, are important.
Fluorescein angiography is useful in identifying structural changes. However, OCT, a non-invasive alternative, can provide more detail on structural changes, including characterizing the artery emboli. Therefore, management should include retinal photos, OCT and close monitoring with weekly follow-up visits scheduled for patients who have acute BRAO, and 12 weeks for chronic disease for the rare complication of retinal neovascularization.
BRAO is a time-sensitive condition, and is best treated immediately to prevent permanent vision loss. Although there is not a single proven modality of treatment, many local therapies have been attempted. These include ocular massage (See “Back to Basics,” page 24) to dislodge the emboli, reducing the IOP, paracentesis and the retrobulbar injection of antivascular agents. There are anecdotal reports of success with ocular massage and paracentesis, but no sound evidence of efficacy.
CLEARING THE BLOCKAGE
BRAO is a significant condition associated with a number of life-threatening systemic diseases. O.D.s play a vital role in not only the early diagnosis and prevention of visual complications, but also in identifying those conditions that may require referral for immediate treatment. OM

| SHERROL A. REYNOLDS, O.D., F.A.A.O., is an associate professor at the Nova Southeastern University College of Optometry and clinical preceptor/attending in the college’s diabetes and macular clinic. She is a fellow of the Optometric Retina Society and chairperson for the Florida Optometric Association Healthy Eyes Healthy People Committee. Comment at tinyurl.com/OMcomment. |