


ICD-10 IMPLEMENTATION
JOHN RUMPAKIS, O.D., M.B.A.
OCTOBER 1 IS FAST APPROACHING, SO IF YOU HAVEN’T STARTED, THE TIME IS NOW
Online Exclusive!
TO VIEW THIS ARTICLE IN ITS ENTIRETY, VISIT US ONLINE:
optometricmanagement.com
THE ADOPTION and implementation of the Affordable Care Act (ACA) has changed the foundation of how healthcare is delivered in the United States by practitioners of all disciplines. As many features of the ACA are rolled out throughout the next few years, the healthcare system is preparing for one of the biggest challenges it has faced in decades: the overwhelming task of transitioning from the ICD-9 coding system to the ICD-10 system.
The ICD-10 original implementation date of 2011 has been pushed back many times, but the date of October 1st, 2015 seems to be firm and non-negotiable as of this writing. There is no grace period, or phase in; it will be an instant transition. And, because the transition to ICD-10 is required for everyone covered by HIPAA, it means most likely that it is going to affect you.
The questions, of course, are: Why this change is happening?, How will it be different?, and What can I do to prepare my practice? Let me help pave the way.
WHY NOW
The impetus to move from ICD-9 to ICD-10 comes from many different forces. Simply put, ICD-9 is 30 years old, and is outdated. Many of the diagnostic categories are full and cannot be expanded to add new entries. And, for those categories and diagnoses that do exist, many are not descriptive enough. Specifically, ICD-9-CM includes about 14,000 diagnosis codes. Under ICD-10-CM, there will be about 68,000 codes. The number of procedure codes will increase from some 3,800 under ICD-9 to about 87,000 under ICD-10.
COSTS VS. BENEFITS
Originally estimated at $83,290 for a small (i.e., three-doctor) practice, in 2008, the U.S. Department of Health and Human Services estimated that the overall cost of converting to ICD-10 would amount to $1.64 billion throughout at least six years.1,2 However, costs have likely increased, as estimated in a 2014 update study by Nachimson Advisors, LLC. (See “Cost Impact of ICD-10” sidebar, page 23).
Regardless of these costs, it is still predicted that the savings to the healthcare system will far outweigh the costs and the long-term benefit to the solvency of the healthcare system will be immense.
According to the U.S. Department of Health and Human Services (HHS), the major benefits of switching to the ICD-10 system include:
• More accurate payments for new procedures.
• Fewer rejected claims.
• Fewer improper claims.
• Better understanding of new procedures.
• Improved disease management.
• Better understanding of health conditions and healthcare outcomes.
• Harmonization of disease monitoring and reporting worldwide.
According to the 2004 RAND Study, “The Costs and Benefits of Moving to the ICD-10 Code Sets,” high-end costs to implement the ICD-10 system averaged approximately $1.5 billion.4 However, the benefits will be a gateway to accurate payment for new procedures, fewer rejected claims, fewer fraudulent claims, better understanding of new procedures and improved disease management, with an estimated benefit throughout a 10-year period of more than $6 billion to the healthcare industry. Though this study is more than a decade old, the data analytics are a major focus within the ICD-10. Combining much higher levels of specificity in combination with better analytics of the EHR and meaningful use measures mean that providing more medically necessary care, faster and for a lower cost is something that is a major objective and benefit of this move.
| Cost Impact of ICD-10 for a Small Practice (2008) | |
|---|---|
| Education | $2,405 |
| Process analysis | $6,900 |
| Changes to superbills | $2,985 |
| IT costs | $7,500 |
| Increased documentation | $44,000 |
| Cashflow disruption | $19,500 |
| Total | $83,290 |
| Cost Impact of ICD-10 for a Small Practice (2014)3 | ||
|---|---|---|
| Training | $2,700 ‐ $3,000 | Pre-implementation total $25,560 ‐ $105,506 |
| Assessment | $4,300 ‐ $7,000 | |
| Vendor/software upgrades | $0 ‐ $60,000 | |
| Process remediation | $3,312 ‐ $6,701 | |
| Testing | $15,248 ‐ $28,805 | |
| Productivity loss | $8,500 ‐ $20,250 | Post implementation total $31,079 ‐ $120,599 |
| Payment disruption | $22,579 ‐ $100,349 | |
| Total costs | $56,639 ‐ $226,105 | |
| Small Practice | Medium Practice | Large Practice | |
|---|---|---|---|
| 2008 estimated costs | $83,290 | $285,195 | $2,728,780 |
| 2014 estimated costs | $56,639 ‐ $226,105 | $213,364 ‐ $824,735 | $2,017,151 ‐ $8,018,364 |
Chapter 7 Codes

|
|
|---|---|
| ICD-10 Codes | Eye Conditions (Categories) |
| H00-H05 | Disorders of the eyelid, lacrimal system, and orbit |
| H10-H11 | Disorders of the conjunctiva |
| H15-H22 | Disorders of the sclera, cornea, iris, and ciliary body |
| H25-H28 | Disorders of the lens |
| H30-H36 | Disorders of the choroid and retina |
| H40-H42 | Glaucoma |
| H43-H44 | Disorders of the vitreous body and globe |
| H46-H47 | Disorders of the optic nerve and visual pathways |
| H49-H52 | Disorders of the ocular muscles, binocular movement, accommodation, and refraction |
| H53-H54 | Visual disturbances and blindness |
| H55-H57 | Other disorders of the eye and adnexa |
| H59 | Intraoperative and postprocedural complications and disorders of the eye and adnexa, not elsewhere classified |
ICD-9 VS. ICD-10
Let’s discuss how ICD-10 will differ from ICD-9.
The ICD-10 book groups diseases and conditions differently than the ICD-9 book. There is greater differentiation by:
• Communicable diseases
• General diseases that affect the whole body
• Local diseases arranged by site
• Development of diseases
• Injuries
• External causes
Chapters 7, 19 and 20 are of primary concern to optometrists. That is not to say that we will not be accessing other chapters on a regular basis; I am only isolating the very essential ones.
Chapter 7 is well organized and delineated for easy reference. Please note that the numeric reference increases as you move toward the back of the eye, so it is fairly easy to start to understand and correlate the numeric value with physical location within the ocular structure. (See “Chapter 7 Codes,” above.)
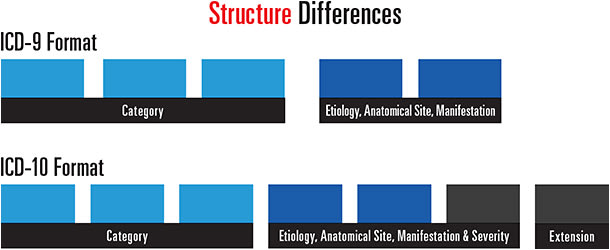
As has been well advertised, the code structure itself will change. With the current ICD-9 diagnosis codes, each code has three to five digits — and most have five because we are obliged to always code to the highest level of specificity. (See “Structure Differences,” below.)
| ICD-9 to ICD-10 Conversion (Examples) | |
|---|---|
| ICD-9 | ICD-10 |
| 367.1 — Myopia | H52.10 — Myopia, unspecified eye |
| H52.11 — Myopia, right eye | |
| H52.12 — Myopia, left eye | |
| H52.13 — Myopia, bilateral | |
| 367.21 — Regular astigmatism | H52.221 — Reg. astigmatism, right eye |
| H52.222 — Reg. astigmatism, left eye | |
| H52.223 — Reg. astigmatism, bilateral | |
| H52.229 — Reg. astigmatism, unspecified | |
| 365.62 — Glaucoma associated with ocular inflammations | H40.40 Glaucoma secondary to eye inflammation, unspecified eye
• H40.40X0 — unspecified stage • H40.40X1 — mild stage • H40.40X2 — moderate stage • H40.40X3 — severe stage • H40.40X4 — indeterminate stage |
| H40.41 Glaucoma secondary to eye inflammation, right eye
• H40.41X0 — unspecified stage • H40.41X1 — mild stage • H40.41X2 — moderate stage • H40.41X3 — severe stage • H40.41X4 — indeterminate stage |
|
| H40.42 Glaucoma secondary to eye inflammation, left eye
• H40.42X0 — unspecified stage • H40.42X1 — mild stage • H40.42X2 — moderate stage • H40.42X3 — severe stage • H40.42X4 — indeterminate stage |
|
| H40.43 Glaucoma secondary to eye inflammation, bilateral
• H40.43X0 — unspecified stage • H40.43X1 — mild stage • H40.43X2 — moderate stage • H40.43X3 — severe stage • H40.43X4 — indeterminate stage |
|
The ICD-10 is organized in a completely different fashion. From a structural basis, an ICD-10 code:
• Is three to seven characters long
• Begins with an alphabetic character (“H” for Eye Section)
• Has a numeral as the second digit
• Includes alpha or numeric digits as the third through seventh characters
• Contains a decimal after first the three characters
• Is not case sensitive
CONVERSION
There are many technologies that will be able to assist in “translating” or converting an ICD-9 code into ICD-10 format. The general equivalence mappings provided by CMS are a great place to start with this, but both commercial programs, such as CodeSAFEPLUS.com, and most EHR programs are already doing real-time conversion. Please understand, though, that in many cases, there is not a simple one-to-one translation. For example, CMS reports that in the “forward” GEMs maps for procedures from ICD-9 to ICD-10 there are 445 instances where a single ICD-9 code can map to more than 50 ICD-10 codes, and 210 instances where a single ICD-9 can map to more than 100 ICD-10 codes. In the “backward” GEMS maps from ICD-10 to ICD-9 there are 6,821 instances in the mappings for diseases where a single ICD-10 code can map back to more than one ICD-9 code, and there are 6,740 instances for procedures where a single ICD-10 code can map back to more than one ICD-9 code.5
Keep in mind, you will maintain both systems in practice for at least one year while this transition is taking place. Generally, healthcare claims can be filed with a third-party insurer up to one year past the date of service. Theoretically, all patients that you provide care for between October 1, 2014 and September 30, 2015 could be filed or re-filed up to September 30, 2016; however, you would have to use the ICD-9 diagnostic codes for these claims, as the ICD-10 wouldn’t have been enforced yet.
One of the biggest changes with the implementation of the ICD-10 is that O.D.s will have to have much greater interaction with the medical record and choose the specific ICD-10 code, particularly in cases where there is a one to many translation. (For common examples, see “ICD-9 to ICD-10 Conversion.”)
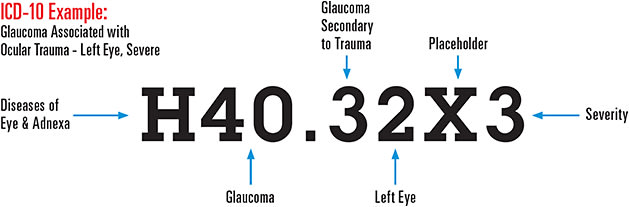
For example, if you were to look at a specific disease state, such as glaucoma, it is easy to see how the ICD-10 code is much more specific and descriptive than the ICD-9. (See “ICD-10 Example: Glaucoma Associated with Ocular Trauma - Left Eye, Severe).
INJURIES AND TRAUMA
Injuries and trauma (chapter 19) will be done much differently than in the ICD-9 system. Chapter 20 will be used in conjunction with 19 to indicate the cause of the injury.
In general, injuries are organized by anatomical site, then type of injury. Also, the seventh character is required to specify status of the encounter (initial vs. subsequent or follow-up). In fact, the seventh character is critical, as it specifies the stage of treatment as follows:
• A - Initial encounter. This describes the entire period in which a patient is receiving active treatment for the injury, poisoning or other consequences of an external cause. So, you can use “A” as the seventh character on more than just the first claim. In fact, you can use it on multiple claims.
• D - Subsequent encounter. This describes any encounter after the active phase of treatment, when the patient is receiving routine care for the injury during the period of healing or recovery.
• S - Sequela. The “S” indicates a complication or condition that arises as a direct result of an injury. An example of a sequela is a scar resulting from a burn.
As you can see from the examples in “The Seventh Character” sidebar (page 27) for very typical types of ocular trauma encountered on a daily basis, the coding in ICD-10 is much more specific than in ICD-9.
However — and this is a significant however — similar to ICD-9-CM, there is no national requirement for mandatory ICD-10-CM external cause code reporting. Unless you are subject to a state-based external cause code reporting mandate or these codes are required by a particular payer, you are not required to report ICD-10-CM codes found in chapter 20 of the ICD-10-CM, External Causes of Morbidity.6
I would encourage you, however, to get in the habit of doing it anyway, as it will most likely be required at some point in the future.
| The Seventh Character | |
|---|---|
| ICD-9 | ICD-10 |
| 930.0 — Corneal foreign body | T15.01XA — Foreign body in cornea, right eye, initial encounter |
| T15.01XD — Foreign body in cornea, right eye, subsequent encounter | |
| T15.01XS — Foreign body in cornea, right eye, sequela | |
| 918.1 Superficial injury of cornea | S05.01XA — Injury of conjunctiva and corneal abrasion without foreign body, right eye, initial encounter |
| S05.01XD — Injury of conjunctiva and corneal abrasion without foreign body, right eye, subsequent encounter | |
| S05.01XS — Injury of conjunctiva and corneal abrasion without foreign body, right eye, sequela | |
| Cause of Injury (Chapter 20) | |
| Tree branch | W22.8XX(A,D or S) — Striking against or struck by other objects, initial (A), subsequent (D) or sequela (S) |
| Fingernail | W50.4XX(A, D or S) — Accidental scratch by another person, initial (A), subsequent (D) or sequela (S) |
ICD-10 IMPLEMENTATION
Though the intricacies can be confusing, the switch to ICD-10 is doesn’t have to be. The key is a proper strategy and path of implementation. Here are 10 steps for a successful implementation within the next 90 days.
1. Review how to take a case history and chief complaint so it will be more detailed and consistent with the increased specificity required by the ICD-10. Keep in mind the maxim “what, where, when, and how” in your recording process.
2. Print out your “Top 30” ICD-9 codes from your EHR in descending order of frequency.
3. Separate your “Top 30” into “Appropriate Categories”:
a. Refractive status
b. Adnexa and lids
c. Conjunctiva
d. Cornea
e. Iris
f. Ciliary body
g. Glaucoma
h. Vitreous
i. Retinal
j. Injury and trauma
k. Systemic
4. Using your conversion algorithm, begin creating a learning tool for each of your “Top 30.” For example, Myopia 367.1 (ICD-9) – H52.11, H52.12, H52.13, H52.10 (ICD-10). Create a timetable for each specific category that you created to provide adequate learning time.
5. Develop a testing system to ensure accuracy at all levels within the practice, physician or staff.
6. Contact your EHR vendor to ensure that it has the proper “end to end” testing completed and verified.
7. Contact your electronic billing “clearinghouse” to ensure that it is equipped to communicate the ICD-10s by Oct. 1, 2015.
8. Verify with your contracted carriers, both refractive and medical, that they are ready to accept ICD-10s by the deadline.
9. Be prepared to maintain both systems in parallel until 2016. Keep in mind, the ICD-9s are not going to go away until September 30, 2016, and will need to be used to retroactively bill for dates of service prior to Oct. 1, 2015.
10. Develop office strategy for change management. Remember, rules and requirements change frequently, so be sure to stay informed on the latest updates.
A BUMPY ROAD TO A BRIGHT FUTURE
There’s no doubt in anyone’s mind that our industry is a dynamic one. The world of coding is no different. Change occurs on a daily basis, whether it’s a reimbursement value, a new rule or regulation or interpretation thereof that places the practitioner at risk. The change to the ICD-10 is primarily about changing to an updated system that will provide the specificity required for “big data” analysis and algorithms to provide more accurate reporting of the actual care required and provided, and the economies of scale to provide cost data based upon episodes of care on a per-diagnosis basis.
There is no doubt in this author’s mind that the ICD-10 is but the first step to the commoditization of physician services — big business metrics applied to the care that is provided on a daily basis, calculated to the penny and with controlled distribution.
They say that the path of change is a bumpy one. The U.S. healthcare system will certainly encounter many potholes as we transition from ICD-9 to ICD-10. But, in the end, we will have a system that is more accurate, more descriptive, allows for more accurate cost analysis and reimbursements, and keeps us, as a country, current on the world stage. OM
REFERENCES
1. The Impact of Implementing ICD-10 on Physician and Clinical Laboratories. Available at http://www.nachimsonadvisors.com/documents/icd-10%20impacts%20on%20providers.pdf. Accessed May 13, 2015.
2. Conn J. ICD-10 Estimated to Cost Vendors, Providers Billions. Available http://www.modernhealthcare.com/article/20080822/NEWS/738760. Accessed May 13, 2015.
3. Hartley C. and Nachimson S. The Cost of Implementing ICD-10 for Physician Practices — Updating the 2008 Nachimson Advisors Study. Available http://docs.house.gov/meetings/IF/IF14/20150211/102940/HHRG-114-IF14-Wstate-TerryW-20150211-SD001.pdf. Accessed May 13, 2015.
4. Libicki M. and Brahmakulam I. The Costs and Benefits of Moving to the ICD-10 Code Sets. Available http://www.rand.org/content/dam/rand/pubs/technical_reports/2004/RAND_TR132.pdf. Accessed May 13, 2015
5. Jones, L. M., and Nachinsom, Stanley. Use Caution When Entering the Crosswalk: A Warning About Relying on GEMs as Your ICD-10 Solution. Available http://www.cms.org/uploads/ICDLogicGEMSWhitePaper.pdf. Accessed May 13, 2015.
6. ICD-10-CM/PCS Myths and Facts. Available https://www.cms.gov/Medicare/Coding/ICD10/downloads/ICD-10MythsandFacts.pdf. Accessed May 13, 2015.

| JOHN RUMPAKIS O.D., M.B.A. is founder, president and CEO of Practice Resource Management, Inc., a consulting, appraisal and management firm for healthcare professionals. Email him at John@PRMI.com, or visit tinyurl.com/OMcomment to comment on this article. |