


CLINICAL
the front
Eradicate Epidemic Keratoconjunctivitis
Identify and cure this highly contagious form of pink eye
JOSH JOHNSTON, O.D., F.A.A.O., ATLANTA
A 16-year-old white female recently presented with a complaint of “pink eye” OD, which she said she had for about a week and was not improving on the antibiotic drops her family doctor prescribed. She said her eye had become “red and swollen” with “excessive tearing.” In addition, she told me she believed her left eye was starting to develop the same condition. Further, she mentioned her friends at school had “pink eye.” Her case history was highly suspicious for epidemic keratoconjunctivitis (EKC), and examination confirmed this diagnosis.
Here, I discuss the etiology, symptoms, clinical signs, management options as well as the ICD-9 codes associated with EKC.
Etiology
EKC is a highly contagious viral conjunctivitis that comes from the adenovirus and occurs via the direct contact of ocular and respiratory secretions. It can survive on inanimate surfaces, such as towels and doorknobs, for four to five weeks, and it is resilient against disinfection, making antibiotics unsuccessful.
Typically, the infection begins in one eye and spreads to the fellow eye in three to seven days. Patients are considered contagious when the eye is inflamed with hyperemia and serous discharge is present. Patients can shed the virus and cause transmission for up to 14 days after the onset of initial symptoms.
ICD-9 or CPT Codes
• 372.00 acute conjunctivitis, unspecified
• 372.02 acute follicular conjunctivitis
• 372.30 conjunctivitis, unspecified
Due to EKC’s exceptionally contagious nature, epidemics are common in schools and at work environments and can easily spread in eyecare offices if infected patients are not handled properly. In my practice, we have a red eye protocol, which consists of placing these patients in a designated exam room, using disposable medical gloves and sterilizing all instruments, the exam chair, doorknob and check-in clipboard with hospital-grade sterilization wipes.
If an early diagnosis is not made or the condition is not properly treated, EKC patients can develop corneal infiltrates around one to two weeks, which can turn into residual scars in the stroma of the cornea, causing permanent decreased vision. The good news: Point-of-care diagnostic tests can confirm a viral etiology. They have a reported 90% sensitivity and 96% specificity, take roughly two minutes to perform and provide results in about 10 minutes.
Symptoms
• Acute onset of tearing
• Decreased vision
• Foreign body sensation
• Light sensitivity
• Ocular itching or burning
Clinical signs
• Conjunctival edema
• Conjunctival injection
• Hyperemia
• Inflammation
• Lid edema
• Palpable ipsilateral preauricular adenopathy
• Peri-orbital edema
• Red eye
• Serous discharge
• Sub-epithelial infiltrates
• Submandibular lymphadenopathy
• Superior petechial hemorrhages
Management options
Currently, no treatments are FDA approved for EKC. The off-label treatments include:
• Palliative treatment. This is for patients who don’t have pseudomembrane or symptomatic subepithelial infiltrates. It consists of cool compresses for five minutes, b.i.d. or q.i.d. to improve discomfort, artificial tears as needed, also to improve discomfort, and combination OTC vasoconstrictors and antihistamines.
• 5% povidone-iodine sterile ophthalmic prep. This has a broad antimicrobial spectrum. After a topical anesthetic is given to the patient, a topical NSAID or steroid is placed on the eye to help decrease burning and discomfort, and four to five drops of the 5% povidone-iodine sterile ophthalmic prep is instilled into the eye(s) for roughly 60 seconds. Next, an irrigating eyewash is employed to remove any residual povidone-iodine. Topical NSAIDs are given after the in-office procedure to relieve pain.
• Combination therapy. I prescribe this regimen for patients who have pseudomembrane or symptomatic subepithelial infiltrates. It consists of cool compresses for five minutes b.i.d. or q.d., artificial tears as needed, topical steroids q.d. to q.i.d to suppress the inflammation of the pseudomembrane or symptomatic subepithelial infiltrates (rule out HSV or other infectious etiologies, especially in contact lens patients to prevent further proliferation of an infection with topical steroid use) and the off-label use of ganciclovir 0.15% gel q.i.d, which significantly reduces both the duration and incidence of subepithelial infiltrates with a recovery time of less than eight days. Steroids can help improve the signs and symptoms of this condition, but recent research reveals it enhances adenovirus replication and delays cell shedding from the ocular surface, which postpones adenovirus elimination. These risks might not outweigh using topical steroids in a case of EKC with sub-epithelial infiltrates that can permanently decrease vision. Use caution when prescribing.
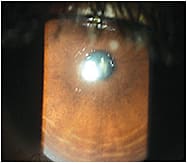
This patient saw the PCP before me. The camera flash constricted the pupil so it looks like the sub-epithelial infiltrate isn’t in the visual axis, but it was.
• Patient education. To help prevent transmission, educate these patients about how EKC spreads from hand to eye contact as well as via airborne respiratory droplets, and instruct them to vigilantly clean commonly touched objects at the office and home with sterilization wipes. Also, advise these patients to be mindful of washing their hands often and every few days, their pillowcases every day and to avoid touching their eye(s). Further, instruct them to keep their distance from family, friends and/or co-workers until the virus has run its course. You may want to advise parents of very young children to keep them home, as little ones are not judicious about hygiene. Finally, tell your contact lens wearers to discard their disposable lenses and only resume wear post-virus.
What’s Coming Up?
• Blepharitis in Review
• HSK
Future treatment options
They are:
• A combination of 0.4% povidone-iodine and 0.1% dexamethasone.
• N-chlorotaurine.
• APD-209 Eye Drops. (See http://1.usa.gov/1aqrfNu).
Bottom line
I prescribed the aforementioned 16-year-old patient combination therapy and explained I was able to identify the real problem via my education and training in eye care and the instrumentation exclusive to eye doctors. Upon one-week follow-up, her EKC resolved. She thanked me and assured that she’d see me first for any future eye problems. OM

| Dr. Johnston practices at Georgia Eye Partners. He focuses on ocular surface disease and has extensive experience in comanaging cataract and refractive surgery patients. E-mail him at drj@gaeyepartners.com, or visit tinyurl.com/OMcomment to comment. |