


UP YOUR GAME WITH PRESBYOPES
A CONTACT LENS WITH AN INNOVATIVE NEW PUPIL-OPTIMIZED DESIGN EXCEEDS EXPECTATIONS WITH MULTIFOCAL WEARERS
Michael Ciszek, O.D.
AS A BIG PRESCRIBER of multifocal contact lenses, I’ll be the first to admit that it hasn’t always been easy to give patients great comfort, great near vision and great distance vision in the same lens. Typically, we had to choose which of those features was least important and compromise a little in that area. From my perspective, that was still a better option than monovision. And most of the time, my patients have been willing to tolerate the tradeoffs for spectacle-free vision.
When 1-DAY ACUVUE MOIST Brand MULTIFOCAL Contact Lenses were first introduced, I was a bit skeptical. But after my first few cases, the skepticism went out the window. This lens has taken my patients from saying, “This is working . . . I’m okay with this” to “Wow, this is fantastic!” In my experience, it works so well for such a broad range of patients that I’ve been switching most of my existing multifocal contact lens wearers — both daily disposable and reusable — into the lens.
Being a daily disposable lens usually means a bigger price tag. But, price hasn’t been much of an issue because of how we position the lens to patients. I let them try the lens and, if they don’t think the benefit is worth the additional cost, there is no harm done; they can stick with their current lenses. However, for most patients, the value — crisp vision at all distances and great comfort — greatly outweighs the costs.
This lens has quickly become my go-to lens for all types of presbyopic patients, from emerging presbyopes to current multifocal to presbyopic spectacle wearers who would benefit from trying multifocal contact lenses. See my top tips for introducing this lens to two of these categories of wearers on page 28.
THE EMERGING PRESBYOPE
If an emmetrope or a single vision contact lens wearer in her late 30s to early 40s mentions anything about eye strain or blur, I trial frame a +1.00 add to see whether she likes it better.
Some doctors don’t test near vision or consider near correction for patients under the age of 40, but I find that with the increased near demands of technology, patients are having problems with convergence and accommodation earlier than they did in the past.
Assuming the patient responds well to the add, I say, “You’re wearing contact lenses because you didn’t want to wear glasses all the time, right? I can give you a lens that has that little bit of reading help that I just showed you incorporated into the lens itself, so you don’t have to wear reading glasses over your contact lenses.” It’s a really easy conversation.
This lens is a great lens to put on these younger patients. I tell them not to expect much change in how they see, but more in how they feel.
Here’s how I explain it: “That small adjustment made it easier for you to read for 20 seconds. Just imagine how much better your eyes will feel getting that near vision help all day long.”
It’s also nice to know that patients will be able to continue in this lens for many years as presbyopia progresses, simply by changing the add combination.
THE CURRENT MULTIFOCAL WEARER
I have a lot of patients currently in other multifocal contact lenses. When one of these patients comes in for an annual exam, I ask four questions:
• Can you wear your lenses comfortably all day long?
• How is your distance vision?
• How is your computer vision?
• How is your vision for reading or up close?
If a patient can legitimately answer that his lenses are performing great on all four of those measures, then I probably wouldn’t suggest a change. But, hardly anyone is doing great on all four. That makes it easy to say, “I have a new lens that should address the problem you are having.” I’m finding that most of the time, this lens works better than the patient’s current multifocals.
TALK ABOUT TECHNOLOGY, NOT COST
If you ask patients, “Do you want product A for $5 or product B for $10?” they will choose A every time. Wouldn’t you? But if you tell them why a certain lens will meet their needs better or solve a problem for them, it changes the conversation. Now you are talking value, not price.
I like to spend a little time explaining the technology that makes a more expensive lens worth the money. Being “new” is not enough of a benefit.
For example, when introducing these lenses, I tell patients that advanced technology helps it center well over the cornea, and I explain pupil optimization in layman’s terms: “In some people, the pupil is a little larger or smaller than normal. So, if the lens is designed for a 7.0mm pupil and you have a 4.0mm pupil, you are missing all that vision around the edges. It’s better to have a lens that is designed to closely match the pupil size we expect for people your age with your prescription.”
USE THE FITTING GUIDE
I don’t usually use fitting guides, but I use the fitting guide for 1-DAY ACUVUE MOIST MULTIFOCAL because it works (see below). In fact, if you try to fit this lens like you fit other multifocals, you may run into problems.
That’s because we’ve all become accustomed to using little tricks to compensate for the flaws in older multifocal lens technology: We over-minus the distance in the dominant eye and under-minus it in the nondominant eye to provide mini-monovision. The lens has such good optics and centration that it already provides the full range of vision it’s supposed to — without the workaround.
Avoiding Common Mistakes
• Incorrect distance refraction or add power
• DON’T over-minus for distance or over-plus for near — +0.75 over should blur out the best acuity line
• DON’T use an old contact lens prescription
• DO obtain a new, functional (maximum plus) distance refraction
• DO determine an appropriate functional add (minimum plus to functional vision for essential tasks)
• Multiple re-fits or low fit success rate
• DON’T follow the fit guide from a different brand
• DON’T refract in the dark
• DO perform a modified Humphriss over-refraction
• Dissatisfied patient
• DON’T promise to solve everything with a contact lens
• DO set proper expectations for task-related spectacle wear in some situations as patients age
• DO consider separate prescriptions for “work” and “play”
We saw this same trajectory with progressive spectacle lens technology. Early progressives weren’t very good at getting the full add into the lens, so optometrists got in the habit of just prescribing 0.25D more plus. With newer designs, we stopped doing that. The bottom line is that the fitting guide is the best way to determine the starting pair and any adjustments that need to be made. I rarely make more than one small change in one eye.
BEST PRACTICES
You need to start with a good refraction and add power determination (see “Avoiding Common Mistakes”). Although there are rough age guidelines, I feel it’s important to test patients’ near vision, and I like to use fused cross-cylinder over their distance prescription to determine the add. This is a quick way to test their accommodative ability in conjunction with their eye posture, or convergence.
This lens needs to settle for about 10 minutes and its performance is best determined in the real world, not the exam lane. Some doctors have patients wait and then test it out by looking across the parking lot and down at their smart phone. Because of the way my work flow is set up, I usually send them home with trial pairs based on the fitting guide and I advise them, “Don’t judge these by the first few minutes!” Then, I make any needed adjustments at the one-week check.
IMPROVING VISION
Through the years I’ve been surprised by how often patients tell me their previous doctor never even mentioned multifocal contact lenses. I see these lenses as a great way to build patient loyalty and generate referrals. Fitting multifocals allows us to retain contact lens wearers as they age and attract new wearers who become presbyopic and prefer not to wear glasses (Figure 1, page 27).
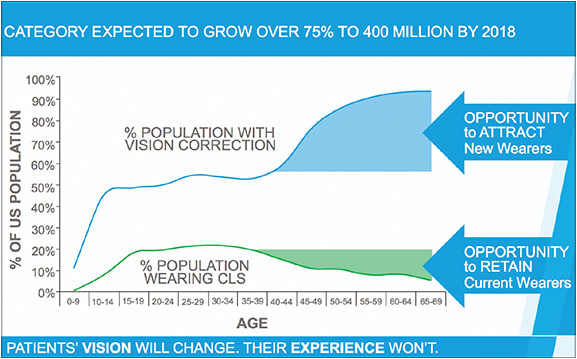
Figure 1: Fitting multifocals keeps patients in contact lenses as they age and attracts new wearers as well.
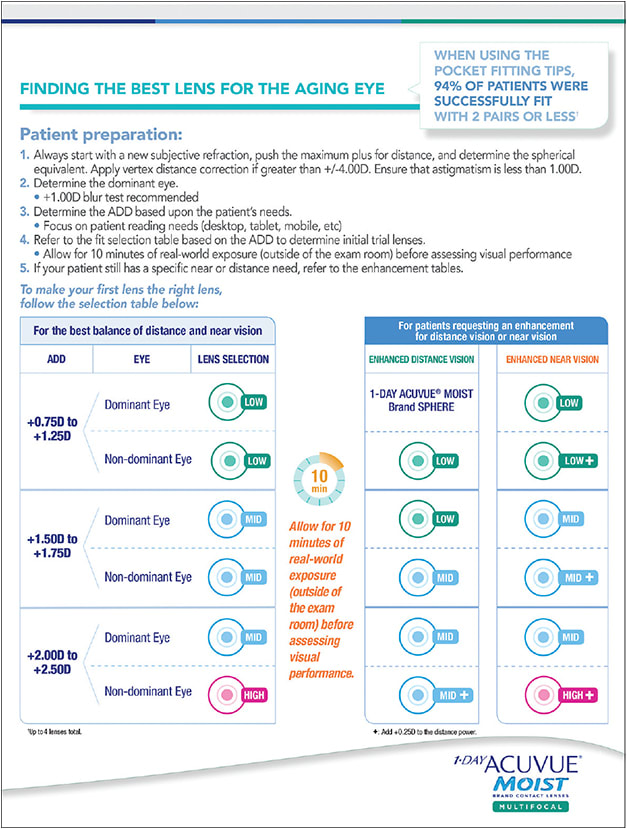
Figure 2: A four-page fitting guide is available to help O.D.s successfully fit the lens.
There is minimal risk to re-fitting current multifocal wearers in these lenses or trying it on emerging presbyopes. In the worst-case scenario, the patient doesn’t see any benefit over their current lenses. But in many cases, you can bring them new technology with the potential to improve their quality of life — and make you look like the hero. OM
Spotlight on Science
The Innovation Behind a Brand New Multifocal
Kurt Moody, O.D., F.A.A.O., F.B.C.L.A.
New 1-DAY ACUVUE MOIST Brand MULTIFOCAL Contact Lens is a center-near continuous aspheric lens that was designed from the ground up, based on data from thousands of successful lens fits.
It addresses the natural variation in pupil size based on age and refractive power, designed to provide consistent performance across adds and refractive range.
This design feature came from research showing that anatomical differences in presbyopic patients drive differences in fit success. For example, it is well known that pupil size decreases with age. Less well known is the fact that there is a very consistent, natural variation of pupil size by refractive status, with myopes having larger pupils than hyperopes, and high myopes having larger pupils than low myopes (Figure 1). In fact, the difference in pupil size by refractive status, based on area, can be as high as 24%.
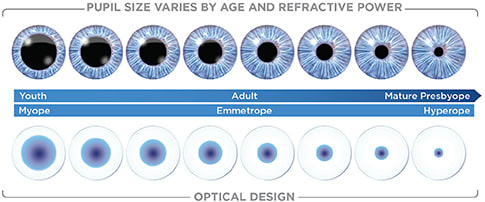
Figure 1: For illustrative purposes only.
Because of their complex optics, the success of multifocal lenses is greatly influenced by pupil size. If the pupil is larger or smaller than the optical design of the lens, for example, the image quality will be reduced. That’s why a single optical design just won’t work for every presbyope.
So, we’ve created 183 unique optical designs. This sounds like an intimidating number, but it actually means that the work of figuring out the best combination has been done already. Now, for the first time, each trial lens will deliver a similar retinal image because of the pupil optimization. For every power/add combination, from +6.00D to -9.00D in 0.25D steps, the lenses are designed to optimize visual performance across ~95% of the range of pupil sizes expected for any given refractive error and add power. The result will be consistent performance across the adds and across the refractive range. That means hyperopes will be as successful as myopes, and the lens is a product your patients will continue to enjoy as their presbyopia advances.
HYBRID BACK-CURVE DESIGN
Lens centration also becomes a critical factor with more complex multifocal optics. The hybrid back-curve design of the lens relies on an aspheric center, as well as low modulus, to help it drape well on the cornea, preserving the integrity of the front-surface optics. Meanwhile, the spherical periphery of the back curve helps maintain centration.
The lens has a base curve of 8.4 with a 14.3-mm diameter, but the unique design gives it a very flexible fit profile. In clinical studies, normal eyes with Ks between 38.75D and 48.50D could be successfully fit with a single base curve.
PROVEN PLATFORM
The etafilcon A material has a 30-year track record of success in delivering comfortable lens wear and crisp vision to millions of patients around the world. The proven material of the 1-DAY ACUVUE MOIST Family of Lenses uses dual-action technology to keep moisture in and irritation out, which helps to address the essential needs of the aging eye:
• LACREON Technology to lock moisture in
• An INFINITY EDGE Design and low modulus to minimize mechanical irritation
• A unique ability to attract and maintain the protein/enzyme lysozyme in its beneficial natural state§
• Class 2 UV blocking†*
The combination of this new and innovative presbyopia-correction technology with the comfortable, easy-to-fit 1-DAY ACUVUE MOIST Platform means that this lens sets doctors and their patients up for success. In fact, when using the fitting tips, 94% of patients are successfully fit with the lenses in just two pairs or less.

| Kurt Moody, O.D., F.A.A.O., F.B.C.L.A., is Global Platform Director, Presbyopia Research & Development for Johnson & Johnson Vision Care, Inc. |
§Data on file, 2014. Based on in-vitro data; clinical studies have not been done directly linking differences in lysozyme profile with specific clinical benefits
†Helps protect against transmission of harmful UV radiation through the cornea and into the eye.
*WARNING: UV-absorbing contact lenses are NOT substitutes for protective UV-absorbing eyewear, such as UV-absorbing goggles or sunglasses, because they do not completely cover the eye and surrounding area. You should continue to use UV-absorbing eyewear as directed. NOTE: Long-term exposure to UV radiation is one of the risk factors associated with cataracts. Exposure is based on a number of factors such as environmental conditions (altitude, geography, cloud cover) and personal factors (extent and nature of outdoor activities). UV-blocking contact lenses help provide protection against harmful UV radiation. However, clinical studies have not yet been done to demonstrate that wearing UV-blocking contact lenses reduces the risk of developing cataracts or other ocular disorders. Consult your eye care practitioner for more information.
See page 4 for more important prescribing information.

| MICHAEL CISZEK, O.D., is in private practice at Visionary Eye Care, with two offices in Chicago. He received compensation from Johnson & Johnson Vision Care, Inc., for his time in writing this article. Visit tinyurl.com/OMcomment to comment on this article. |