


CLINICAL
POSTERIOR
CLASSIFY THIS CLOG
CAN YOU FIGURE OUT WHAT CAUSED THIS PATIENT’S SUDDEN BLURRED VISION?
SHERROL A. REYNOLDS, O.D., F.A.A.O.
A 53-YEAR-OLD black female with hypertension and hypercholesterolemia presented with sudden, painless loss of vision OS upon waking. She confessed non-compliance to her hypertension medication. Her BCVA was 20/20 OD and 20/200 with no improvement on pinhole OS. Pupils were sluggish with a mild afferent pupillary defect (APD) OS. Ocular motilities were unremarkable, but confrontation visual field showed a field defect OS. IOPs were 18 mmHg OD and OS. In-office blood pressure was 160/100 mmHg.
Dilated evaluation OD revealed a healthy optic nerve and normal retinal findings. Evaluation OS showed hyperemia and swelling of the optic nerve, extensive hemorrhages involving the posterior pole and her peripheral retina and dilated and tortuous retinal veins. Also, SD-OCT OS showed multiple intraretinal cystic changes and a serous foveal detachment. Fluorescein angiography was not performed at this visit, but performed by a retinal specialist at a later visit.
Branch retinal vein occlusion and hemi-retinal vein occlusion were ruled out. So, were this patient’s symptoms and clinical findings due to ischemic or non-ischemic central retinal vein occlusion (CRVO)?
Here, I discuss the etiology, symptoms, clinical signs and diagnosis/management of CRVO to help you classify this clog.
ETIOLOGY
Other than diabetic retinopathy, CRVO is the most common sight-threatening retinal vascular disease, according to Archives of Ophthalmology. The majority of CRVO patients are older than age 50, with men slightly more affected than women.
Major risk factors for CRVO are metabolic syndrome (hypertension, diabetes mellitus and hypercholesterolemia) and glaucoma or ocular hypertension. Other risks: oral contraceptive or hormone use, smoking, obesity, sleep apnea and inflammatory (e.g. sarcoidosis) and hematological disorders (e.g. leukemia). CRVO that is bilateral, occurs in younger patients or has atypical features (see “Clinical signs”) should prompt further investigation for thromboembolic disorders, including protein C or S deficiency, antiphospholipid syndrome and hyperhomocysteinemia.
CRVO results from thrombosis within the central retinal vein at or posterior to the lamina cribrosa due to a combination of factors, including endothelial cell wall damage, increased blood viscosity and abnormal platelet formation. The result is elevated intraluminal pressure within the capillaries, triggering hemorrhages and leakage that further impede capillary perfusion and lead to ischemia. Retinal ischemia subsequently leads to the production of vascular endothelial growth factor (VEGF) and inflammatory mediators that, in turn, induce macular edema and neovascularization, according to The New England Journal of Medicine.
There are two types of CRVO, ischemic (greater than 10-disc areas of capillary non-perfusion observed on fluorescein angiography) or non-ischemic (perfused), each with a different prognosis and treatment. Non-ischemic CRVO accounts for a majority (83%) of cases and is less serious than the potentially blinding ischemic type, according to the American Journal of Ophthalmology.
SYMPTOMS
Symptoms vary depending on type, severity and chronicity. So, patients may complain of sudden, painless loss of vision, they may express concern over mild vision loss, transient episodes of blurring, metamorphopsia and central scotoma, and some may be asymptomatic.
CLINICAL SIGNS
• VA (ischemic: VA 20/200 or worse/non-ischemic: VA 20/200 or better)
• Pupils (ischemic: marked APD/non-ischemic: mild-no APD)
• Visual field defects
• Dilated tortuous veins
• Flame hemorrhages
• Dot and blot hemorrhages
• Cotton wool spots
• Hard exudates
• Retinal edema
• Macular edema (the leading cause of vision loss in CRVO)
• Ischemic maculopathy
• Retinochoroidal collateral vessels (indicates prior CRVO)
• Neovascularization (iris angle, retina or neovascular glaucoma)
• Vitreous hemorrhage
• Optic atrophy
DIAGNOSIS/MANAGEMENT
In addition to obtaining a thorough medical history, checking the patient’s blood pressure and obtaining a medical work-up for the aforementioned conditions, the following tests should be used to aid clinicians in the proper diagnosis of CRVO:
• Amsler grid and visual field test. The Amsler grid can enable the identification of metamorphopsia and central scotoma. Automated perimetry is useful in quantifying the visual field defects observed in CRVO patients.
• Macular microperimetry. This allows for specific testing of macular sensitivity and function, resulting from macular edema or ischemia and, therefore, may be considered.
• Gonioscopy. Ischemic CRVO is associated with a higher risk of neovascularization of the iris and angle, potentially leading to elevated IOP and neovascular glaucoma (NVG). The phrase “90-day glaucoma,” is used to monitor for NVG developments, as NVG typically occurs one to four months after CRVO onset. It is essential that careful gonioscopy be done monthly for the first three months.
• Fundus autofluorescence (FAF). This can be a helpful tool in identifying the severity and monitoring treatment of CRVO macular edema hyperautofluorescence. It can detect patchy ischemic retinal whitening near the macula, which is seen as perivenular hypoautofluorescence or a fern-like appearance.
• Retinal photography. This this test is needed to document clinical findings and changes through time, as well as for patient education.
• SD-OCT. Use this to assess for macular edema or ischemia and monitor the course of the disease and treatment response. Poor visual outcome is observed with loss of foveal inner segment and outer segment junction line and absence of inner retinal layers in late-stage SD-OCT images.
To detect microvascular network damage, such as capillary non-perfusion or leakage, in CRVO, optical coherence tomography angiography is a new technology that can aid in this detection.
• Fluorescein angiography (FA). FA is an essential tool for the evaluation of disease severity, visualizing capillary non-perfusion, macular edema and ischemia.
• B-Scan ultrasonography. This is a valuable test when media opacity, such as cataracts, is present, to help detect CRVO complications, such as vitreous hemorrhage.
• Electroretinography (ERG). ERG can help differentiate ischemic from non-ischemic CRVO by showing a decreased b-wave amplitude due to ischemic disease.
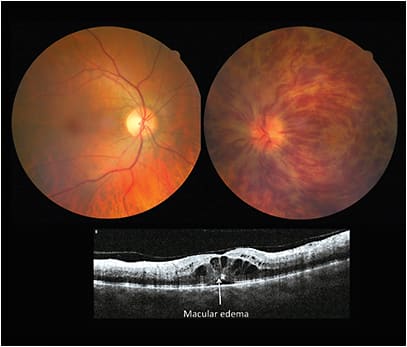
Note this patient’s macular edema.
The management of CRVO includes differentiating the two types, follow-up observation and continuous care. In fact, the central vein occlusion study recommends close follow-up (every three to four weeks) and gonioscopy and undilated slit lamp examination of the iris.
Non-ischemic CRVO may resolve completely without complication. However, some eyes may convert to the ischemic type, which occurs within the first four months of onset. The prognosis is poor in ischemic CRVO. In more that 90% of cases, final VA may be 20/200 or worse. Also, anterior segment neovascularization, with associated NVG, develops in more than 60% of cases, according to Survey of Ophthalmology. This can happen within a few weeks and up to one to two years afterward.
If, however, the patient’s vision deteriorates, macular edema exist or worsen, neovascularization develops or he or she has or develops ischemic CRVO, refer to and co-manage the patient with a retinal specialist. He or she can provide an anti-VEGF injection, which is now considered first-line therapy. Other options include intravitreal steroid injection, focal or pan-retinal laser photocoagulation or pars plana vitrectomy.
THE ANSWER
If you diagnosed this patient with non-ischemic CRVO, you are correct! She was immediately referred to her primary care physician for better blood pressure control. She was co-managed with a retinal specialist and found to have less than a 10-disc area of capillary non-perfusion. Due to the macular edema, she was treated with an intravitreal bevacizumab (Avastin, Genentech) injections OS. At one-month follow-up, her vision improved to 20/40 with reduced macular edema on SD-OCT, and no neovascularization was observed. The patient received additional bevacizumab injections, and her vision stabilized at 20/25 OS with complete resolution of her macular edema, retinal hemorrhages and optic nerve swelling. No neovascularization in the retina, iris or angle developed, and she is being closely monitored with three-month follow-up care.
Improving and preserving vision is critical in cases of CRVO. O.D.s play an important role in the early diagnosis, prompt treatment and patient education of this condition. It is also important for the O.D. to be aware of underlying systemic causes and partner with the patient’s health care provider in the patient’s care. OM

| DR. REYNOLDS is an associate professor at the Nova Southeastern University College of Optometry and clinical preceptor/attending in the college’s diabetes and macular clinic. She is a fellow of the Optometric Retina Society and chairperson for the Florida Optometric Association Healthy Eyes Healthy People Committee. Comment at tinyurl.com/OMcomment. |