


CLINICAL
ANTERIOR
PUT A LID ON MGD
ENABLE PATIENTS TO RECEIVE SYMPTOM RELIEF
JOSH JOHNSTON, O.D., F.A.A.O.
SEVERAL YEARS ago, a 59-year-old male was referred to my dry eye clinic complaining of ocular dryness and redness post LASIK surgery OU. Diagnostic testing revealed evaporative dry eye disease (DED), due to meibomian gland dysfunction (MGD), and aqueous deficiency. I prescribed a treatment regimen of lid hygiene (warm compresses/lid scrubs), artificial tears, cyclosporine ophthalmic emulsion 0.05% drops (Restasis, Allergan), short-term topical corticosteroids and omega-3 supplements.
Through the next three years, the patient returned several times for follow-up visits. At each visit, his symptoms remained. My next course of action was to evaluate him for a thermal pulsation procedure. I conducted a full work-up, including assessing his gland morphology. Turns out the reason the patient’s symptoms remained was because he had lost almost all his meibomian glands due to 10 years of severe MGD prior to seeing me. (At the patient’s initial exam, I did not diagnose severe gland loss because, at that time, gland morphology was not on my radar. Today, this is something I do on a regular basis, thanks to the recent findings of the International Workshop on Meibomian Gland Dysfunction [IWMGD]).
This case illustrates the seriousness of MGD and, therefore, the importance of swift identification and treatment. To aid you, here, I review the etiology, symptoms, clinical signs, management options, associated ICD-10 codes and what happened with this patient. (See “Keep MGD on Your Diagnostic Radar,” page 59.)
| Ulcerative blepharitis | H01.01 |
| Squamous blepharitis | H01.02 |
ETIOLOGY
The IWMGD defines MGD as a “chronic, diffuse abnormality of the meibomian glands, commonly characterized by terminal duct obstruction and/or qualitative/quantitative changes in the glandular secretion.” The condition appears most prevalent in Asian populations (more than 60%).
The IWMGD has proposed classifying MGD into two categories, based on gland secretion: low-delivery (hyposecretory or obstructive, with cicatricial and noncicatricial subcategories) and high-delivery (hypersecretory).
With regard to causes, aging, hormonal changes (androgen deficiency, menopause), medications (antidepressants, antihistamines, drugs for benign prostatic hyperplasia, hormone therapy and retinoids), Sjögren’s syndrome, elevated cholesterol, psoriasis, rosacea and hypertension are associated with MGD.
SYMPTOMS
• Blurred or fluctuating vision
• Burning
• Contact lens discomfort
• Dryness
• Fatigue
• Foreign-body sensation
• Grittiness
• Itching
• Stinging
CLINICAL SIGNS
• Anterior staining at the Marx line (the more anterior the line of the stain, the worse the MGD) of the corneal epithelium
• Biofilm on the lid
• Capped glands
• Chalazia formation
• Conjunctival staining
• Corneal staining
• Decreased TBUT
• Epithelial ridging between gland orifices
• Gland obstruction leading to gland atrophy and loss
• Increased ocular surface inflammation
• Increased tear osmolarity
• Lash loss
• Lid and ocular hyperemia
• Lid inflammation
• Lid telangiectasia
• Poor quality and secretion of meibum
• Redness
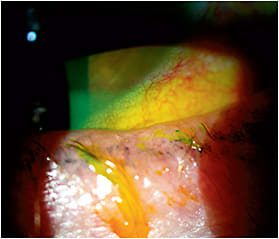
Note the “scalloped” lid margin from gland loss and gland atrophy. You can also see mild saponification, or a foamy tear film. There is also lid telangiectasia, lash loss, misdirected lashes and conjunctival hyperemia.
DIAGNOSIS/MANAGEMENT
The following can be used to diagnose MGD:
• Blink evaluation. Diagnostic equipment is now available to enable you to assess blink quality, so you can determine whether infrequent and/or incomplete blinking is prohibiting the efficient release of meibum.
• Gland expression. This enables you to grade the quantity and quality of the meibum to determine how well the glands are functioning. If they produce a cloudy or toothpaste-like consistency, you are dealing with MGD. Various devices can be used to push on the temporal, medial and nasal lower lids to accomplish gland expression.
• Interferometry. This diagnostic technology measures lipid layer thickness on the pre-corneal tear film.
• Stains and vital dyes. NaFL is instilled and can show punctate keratitis, and it is used to conduct TBUT testing. Lissamine green is instilled to view the conjunctiva and lids under white light, showing staining from dryness. This staining on the lids (Line of Marx) is useful to evaluate MGD. A decreased TBUT with NaFl is believed to be from MGD.
• Lid evaluation. You want to look at the lids for telangiectasia, inflammation, capped glands and a more anterior line of Marx with lissamine green stain and scalloped lid margins.
• Meibography. This is a photo, almost like an X-ray of the glands, to help you see the gland shape, count, function and loss.
• Matrix Metalloproteinase-9 (MMP-9) test. MMP-9 is a proteolytic enzyme and a non-specific inflammatory marker associated with DED. A positive test occurs when there is >40 ng/ml of MMP-9 detected in the tears.
• Tear osmolarity. The concentration of electrolytes in the tear film is measured. High osmolarity numbers >308 and differences between the eyes >8 can indicate DED.
• TBUT? NIBUT. Use these to assess for evaporative DED. To perform TBUT, sodium fluorescein is instilled, and the patient is asked to cease blinking for as long as possible. The tear film is then observed under a broad beam of cobalt blue illumination. TBUT is recorded as the number of seconds that elapse between the last blink and the appearance of the first dry spot in the tear film. A TBUT below 10 seconds is considered abnormal, likely due to MGD.
Keep MGD on Your Diagnostic Radar
The following are red flags for MGD:
• Patients who say, “Wait! Let me blink so I can see” before undergoing a refraction. MGD causes an unstable tear film and limits clarity during refractions. This, in turn, can decrease test accuracy and cause unstable or incorrect spectacle prescriptions, leading to increased spectacle remakes and patients who are not pleased with their quality of vision.
• Patients who present for excessive contact lens appointments. MGD decreases contact lens comfort, wear time and vision, if not identified and treated. This can create unhappy patients, contact lens dropouts and patient/doctor frustration.
• Contact lens dropouts who seek LASIK. Many of these patients seek this refractive surgery because ocular dryness caused them to cease contact lens wear. As we know, LASIK can sometimes worsen DED, so it’s imperative we assess these patients for DED prior to LASIK.
Management for MGD includes:
• Artificial tears. Used to lubricate the ocular surface.
• Cyclosporine ophthalmic emulsion 0.0.5% (Restasis, Allergan). Prescribed to decrease ocular surface inflammation.
• Short-term topical steroids. These decrease inflammation and, therefore, help improve clinical signs and symptoms.
• Lid hygiene (warm compresses/lid scrubs). These are used to achieve and maintain healthy lids and lashes.
• Omega-3 supplementation. These are taken to counteract inflammation that stems from dietary choices.
• Thermal pulsation. A device that uses an algorithm of heat and massage on the inner eyelids to unclog the meibomian glands.
• Amniotic membranes. These help patients who have severe MGD by decreasing inflammation and promoting healing.
• Topical antibiotics. These can improve both the symptoms and clinical signs of MGD when you have more advanced lid disease and, therefore, need treatments that are more effective than lid hygiene and other mild treatments.
Finally, Oculeve, recently purchased by Allergan, has an implant in development that electrically stimulates the lacrimal gland.
THAT PATIENT
The aforementioned patient needed treatment before seeing me to prevent permanent gland loss. In an effort to provide some relief, I treated him with thermal pulsation, which did slightly improve his symptoms. I maximized the function of the glands he had left, but once a gland dies, you can’t bring it back. If caught early enough, you can prevent progression and slow this chronic and progressive disease. OM

| DR. JOHNSTON practices at Georgia Eye Partners. He focuses on ocular surface disease and has extensive experience in co-managing cataract and refractive surgery patients. Email him at drj@gaeyepartners.com, or visit tinyurl.com/OMcomment to comment. |