


CLINICAL
POSTERIOR
AMD PREVALENCE & SUPPLEMENTS
REASONS FOR DIAGNOSIS RISE, WHAT YOU CAN DO ABOUT IT, AND ZINC OR NO ZINC?
SHERROL A. REYNOLDS, O.D., F.A.A.O.
Q: WHY IS AMD ON THE RISE?
A: There are three reasons for this:
1. Rapidly aging baby boomers. Baby boomers, the second largest population behind millennials, began turning age 65 in 2011. This is significant because AMD is the leading cause of permanent impairment of reading and fine or close-up vision among people aged 65 years and older, reveals the CDC. Unfortunately, most don’t realize they have the disease until they suffer vision loss.
2. Increased awareness. Because so many baby boomers have been diagnosed with AMD, awareness of the disease has increased, and this has also contributed to the rise in diagnosis. Further, the widespread use of nutritional support for eye health, particularly lutein and zeaxanthin, and related advertising has also lead to more attention about AMD.
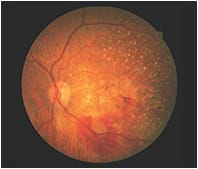
Exudative Wet AMD with subretinal hemorrhage.
3. Advanced technology. Fundus photography, fundus autofluorescence and OCT, in particular, have aided in the early diagnosis of the disease, which has lead to an increase in cases of AMD. Macular Pigment Optical Density has been valuable in identifying at-risk patients as well.
AMD remains a formidable challenge with millions of Americans losing their sight from this condition. To curb its increasing prevalence, we, as optometrists, should determine which patients have modifiable risk factors (smoking, high-intake of dietary fats, uncontrolled hypertension/cholesterol, obesity [BMI>30] and excessive exposure to sunlight and blue light) for the disease, so that we can educate them on the importance of cigarette cessation, dietary changes and wearing ophthalmic lenses that selectively filter or block UV or blue-violet light.
Similarly, risk factors that cannot be controlled, like gender (post-menopausal women are at greater risk) and family and genetic history should be assessed. As early diagnosis is essential, promoting the importance of yearly comprehensive eye exams and follow-up appointments is necessary.
Q: WHEN A PATIENT HAS DRUSENOID MACULAR CHANGES, SHOULD I PRESCRIBE A SUPPLEMENT THAT CONTAINS ZINC?
A: The answer is to use your judgment based on the currently available research. The controversy surrounding zinc and other antioxidants for AMD centers on the relationship with genetic variants, particularly the CFH and age-related maculopathy sensitivity 2 (ARMS2) genotypes. Although the pathogenesis is not well understood, the binding of zinc to CFH can actually increase inflammation and progression to advance AMD, reveals a 2013 study by Carl Awh, M.D. and associates in “Ophthalmology.” The study also shows that patients with ARMS2 were more likely to benefit from zinc-only supplementation.
Another study by Emily Chew, M.D., and associates, also published in “Ophthalmology,” shows no clinically significant interaction between CFH and ARMS2 alleles with zinc and that AREDS supplements reduce the rate of AMD progression across all genotype groups.
Something else to keep in mind is the dosage of zinc: The AREDS 1 formulation contains 80 mg of zinc (8x greater than the recommended daily allowance), thus AREDS 2 compared the effects of lower dose zinc (25 mg) vs. the original 80 mg for any statistically significant differences in progression to advance AMD and found none. Additionally, high doses of zinc can lead to the disturbance of copper metabolism (thus the addition of 2 mg of copper in the AREDS formula), reduced iron function, upset stomach, suppression of immune function and reduced levels of high-density lipoproteins, leading to atherosclerosis, according to the Expert Group on Vitamins and Minerals. The current NEI recommendation is 80 mg of zinc.
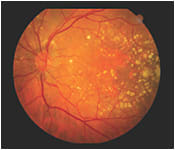
Dry AMD with geographic atrophy
Finally, recent studies suggest that genetic testing of AMD patients may provide clues to nutritional therapy, though more research is needed. Routine genetic testing for AMD, although available, is currently not recommended by the American Academy of Ophthalmology Task Force on Genetic Testing. OM
Questions are based on reader responses to an Optometric Management online survey, which closed on Dec. 20.

| DR. REYNOLDS is an associate professor at the Nova Southeastern University College of Optometry and clinical preceptor/attending in the college’s diabetes and macular clinic. She is a fellow of the Optometric Retina Society and chairperson for the Florida Optometric Association Healthy Eyes Healthy People Committee. Comment at tinyurl.com/OMcomment. |