


FROM THE moment I met John G., a soft-spoken 83-year-old, I could see the look of desperation in his eyes. When I asked what brought him to the practice, he explained that since moving to New England about five years ago, his eyes had become more and more dry and uncomfortable. John further divulged that he’d seen several optometrists, had multiple visits with his primary care doctor, had seen a psychologist and tried “every” artificial tear, doxycycline, an anti-inflammatory drug and punctual plugs (the latter two caused intolerable side effects) without any improvement in his discomfort. “Doc,” he said quietly, “Please. Is there anything you can do to help me?”
In patients who suffer from advanced dry eye disease (DED) like John, we, as optometrists, need to consider using essential fatty acids (EFAs) as a treatment option. Using EFAs as a component of treatment for DED has experienced renewed interest. The thought is that since some consider the etiology of DED to be inflammatory in nature, the use of EFAs, which have been shown to play a role in decreasing inflammatory processes, could potentially help reduce manifestations of DED.
Here, I provide an overview of EFAs, discuss studies that reveal the efficacy of omega-3 supplementation and what, specifically, to prescribe to patients like John.
EFAS
For cells in the body to function properly, many important nutrients are needed, including fatty acids. Fatty acids are the main structural components of fat. Without fat, our bodies cannot operate normally. The body can produce some types of fatty acids called non-essential fatty acids, including stearic acid, lauric acid and oleic acid. Others, called essential fatty acids (EFAs), cannot be synthesized directly from the body and must be obtained from the diet.
The two essential fatty acids that the human body cannot produce are called alpha-linolenic acid (ALA), an omega-3 fatty acid, and linoleic acid (LA), an omega-6 fatty acid. Both fatty acids are necessary for not only growth and repair in the body, but also for conversion to other fatty acids. One example of this conversion: Once eaten, the body is able to convert ALA to eicosapentaenoic acid (EPA) and then to docosahexaenoic acid (DHA). EPA and DHA are important pre-cursors involved in the modulation of inflammatory processes.
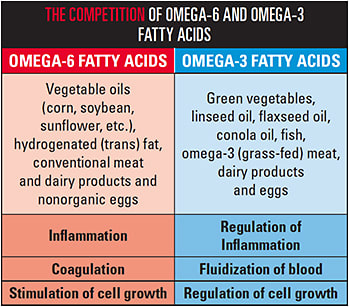
The ratio of omega-6 to omega-3 fatty acids affects the body’s inflammatory status, as omega-6 fatty acids are pro-inflammatory, while omega-3 fatty acids — especially long-chain EPA and DHA — are anti-inflammatory. (See “The Competition of Omega-6 and Omega-3 Fatty Acids,” above.) As a result, researchers recommend this ratio be 4:1 of omega-6 to omega-3, or lower, according to the Sept. 2011 issue of the American Journal of Clinical Nutrition. Unfortunately, the typical American diet contains 10 to 30 times more omega-6 than omega-3, reports the June 2008 issue of Experimental Biology and Medicine. Since research reveals DED is related to inflammation of the ocular surface, it is thought that prescribing omega-3 fatty acid intake would improve tear film integrity and, thus, the symptoms and signs of DED.
EFFICACY
So, do omega-3 fatty acids work as a treatment for DED? Several studies reveal the answer is yes. Here are two examples:
- Dietary omega-3 fatty acid increases resulted in a 30% reduction in the risk of DED symptoms for each 1000 mg of omega-3 consumed daily, reports the October 2005 issue of the American Journal of Clinical Nutrition. Specifically, 40,000 female health professionals studied the lipid composition of the tear film and noted that the ratio of omega-6 fatty acids to omega-3 fatty acids in the tear film was higher in DED patients. The reduction in DED symptoms was thought to be due to the influence of omega-3 fatty acids on the lipid composition of the tears.
- Omega-3 supplements were found to decrease tear evaporation time and increase goblet cell density, leading to a more stable tear film, reports the June 2015 issue of Contact Lens & Anterior Eye. Specifically, the study was carried out on 478 ocular dryness subjects randomized to receive either two capsules per day of omega-3 fatty acid supplements, containing 180 mg EPA and 120 mg DHA, or a placebo. After three months on this regimen, the omega-3 supplement group experienced improvements in TBUT, Schirmer’s test, conjunctival impression cytology and DED symptoms. Further, 70% of them reported freedom from DED symptoms at the end of the three-month period, as opposed to 15% in the placebo group.
PRESCRIBING
In knowing that omega-3 fatty acids are an effective DED treatment, we, as optometrists, can improve severe DED symptoms by offering patients several methods for increasing their omega-3 consumption. Of note: The dietary origin of omega-3 fatty acids is important. Specifically, omega-3 fats from plants, such as walnuts or chia seeds, are rich in ALA, which must first be converted to EPA then to DHA in a series of seven chemical reactions. Thus, more are needed to have an impact on DED symptoms, reports the Feb. 2006 issue of The Proceedings of the Nutrition Society. Omega-3 fats from fish, however, are enriched in EPA and DHA and do not need to undergo the complex conversion of plant-derived omega-3s. Methods for increasing omega-3 consumption:
- Diet modification. Encourage patients to eat more foods rich in omega-3 fatty acids and fewer foods high in omega-6. To increase omega-3 fatty acid intake, recommend patients incorporate oily cold water fish, such as salmon, trout, sardines, mackerel, swordfish, tuna and shellfish, in their diets, as these fish contain high amounts of EPA and DHA. Two servings of cold water fish weekly is the recommended target for both cardiovascular health and DED therapy, reports the July 2011 issue of Current Opinion in Ophthalmology. Patients can expect to see improvement in their symptoms in a matter of 2 to 3 months.
If your patient isn’t a fan of fish, recommend he or she eat walnuts or any type of tree nuts, chia seeds and dark green leafy vegetables, as these food items are also excellent sources of ALA omega-3 fatty acids. Remember, however, ALA omega-3 fatty acids are inefficiently converted to EPA by the body, as mentioned above. Thus, this type of patient would also still likely need an additional source of omega-3 supplementation for optimal DED symptom relief. - Omega-3 ocular nutrition supplements. This is an excellent option if diet modifications are difficult or resisted by patients. That said, always educate patients that symptom relief does not occur minutes or hours after taking the first supplement, but, rather, often comes after months of use. Symptom improvement was noted after three months of supplementation, reports the Dec. 2013 issue of the International Journal of Ophthalmology. Most patients will also still benefit from the combination of omega-3 therapy and other appropriate DED therapies based on their specific presentation of DED. (See “Ocular Nutrition Supplements,” p.27.)
In the United States, uniform fish oil quality standards do not exist. Therefore, individual formulations vary, not only in the levels of EPA and DHA, but also in the molecular structure of the fats in the oil, which impacts absorption and bioavailability. Studies are ongoing to determine the optimal dose, formation and duration of use of omega-3 fatty acid supplements for supreme DED symptom relief. I, typically, start DED patients on 1000 mg per day b.i.d. with a meal. (Omega-3s are fat soluable, just like Vitamin A, D and E, so they must be taken with a good polysaturated fat, such as tree nuts, eggs or Greek yogurt, to aid in absorption.) In patients who have severe DED, I often recommended 3000 mg or more per day.
Ocular Nutrition Supplements
Several companies specialize in ocular nutrition supplements to provide a healthy balance of omega-6 to omega-3 fatty acids and, thus, relief to DED patients.
- Guardion Health Sciences
(Omega Boost DHA Concentrate) - Nordic Naturals
(ProOmega 2000, ProOmega 3.6.9, and ProEPA with Concentrated EPA) - Physician Recommended Nutraceuticals (PRN)
Dry Eye Omega Benefits and Dry Eye Omega Benefits Liquid. - ScienceBased Health
(HydroEye) - ZeaVision
(EyePromise EZ Tears Line)
Be mindful, however of a patient’s current medications. Patients who are on medications known to affect coagulation and platelet aggregation, such as warfarin, may experience bleeding with the addition of omega-3 fatty acid supplementation. In diabetic patients, taking omega-3 supplements may possibly increase fasting blood sugar levels. This was not the case for John. (See “Ocular Nutrition Supplements,” above.)
THE DESPERATE PATIENT
John recently presented for his annual comprehensive exam with a big smile and a new spring in his step. After more than a year of omega-3 supplementation, he is back to doing activities his ocular dryness prevented him from enjoying for years, including enjoying long walks with his wife, mini golfing and ping pong. He reports that he no longer hates New England and that he is finally able to enjoy life again without the symptoms of dry, irritated eyes. OM
