


THE MERIT-BASED Incentive Payment System (MIPS), from CMS, is designed for a specific purpose: controlling costs and changing the way qualified health care providers get paid. While most think that this change won’t affect them, because their Medicare patient volume is low, they are wrong. While it is only CMS that currently has this system in place, assume that eventually every medical health care insurer will also move to a merit-based system of compensating physicians for the care provided to patients, as a result of the overall health care reform move toward value-based medicine. For example, Anthem invested $38 billion into its outcome-based care business to plan for and anticipate the future, according to Forbes.
WHERE DID MIPS COME FROM?
For years, the health care system has monetarily rewarded providers based on the number of tests or procedures performed. The more you did, the more you got paid. We have seen this trickle down from the carriers to the individual companies that provide you with the equipment used to provide care for patients: “Hi, Dr. Smith, if you buy my XYZ piece of equipment, you will only need to perform XX per month, at this reimbursement rate from the insurance carrier to break even. But if you do more, this can be a huge revenue center for the practice…”
This situation is all too familiar, particularly in eye care where ancillary testing is not uncommon. Unfortunately, this model is not sustainable as health care costs are rising at an inflationary rate greater than the general economy, according to “Medical Cost Trend,” a report from accounting firm PricewaterhouseCoopers, now PwC.
The federal government has recognized this and passed legislation for change two years ago. With the passage of the Medicare Access and CHIP Reauthorization Act of 2015, CMS stabilized the current payment system, while directing the Secretary of Health and Human Services to consolidate components of the three specified existing performance incentive programs into a new program — MIPS.
Under this incentive-based system, eligible professionals shall receive annual payment increases or decreases based on their performance, as measured by standards the Secretary shall establish according to specified criteria.
WHY THE SHIFT TO MIPS NOW?
Don’t be afraid of this shift to quality from quantity; it is a natural transition in the evolving business of medicine. All businesses go through phases as an industry matures. The traditional fee-for-service model that CMS adopted at its inception in 1966, hit its 50th anniversary last year. While the model is not that old in business terms, the health care industry is hitting its next business phase of creating efficiencies while maintaining effectiveness. Changing the system that determines what and how we get paid by insurance carriers creates uncertainty and the resultant lack of action that gets us nowhere, but there is a silver lining.
KNOWLEDGE IS POWER
The federal government has done a very good job in outlining exactly what health care providers have to do, when to do it and why to do it, regarding the new MIPS program. By the end of this article, you will have a new favorite website — the CMS Quality Payment Program site: qpp.cms.gov/ . Here, CMS has laid out, in a very pragmatic manner, everything you will need to be successful in being a quality provider.
AM I A PARTICIPANT?
Optometrists, who have been considered physicians under CMS since 1987, are included in this program. You’re part of the Quality Payment Program (QPP), of which MIPS is one track, in 2017 if you bill Medicare more than $30,000 in Part B allowed charges a year and provide care for more than 100 Medicare patients a year. “You must both meet the minimum billing and the number of patients to be in the program,” according to the CMS website. Enter your National Provider Identifier (NPI) into the website for a quick answer on eligibility.
HOW DOES MIPS WORK?
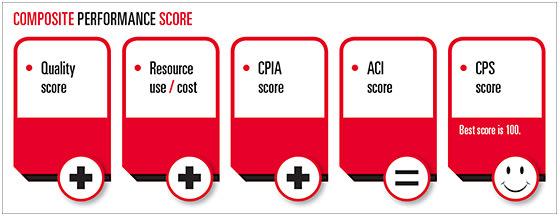
A provider’s positive, negative or neutral payment adjustment will be based on his or her Composite Performance Score (CPS) up to +/-4% in 2019. Four categories of physician performance contribute to your CPS, topping off at 100 points, based on these relative weights:
- Quality (formerly PQRS): 60% for 2017 (50% for following years)
- Advancing Care Information (ACI, formerly meaningful use): 25%
- Clinical Practice Improvement Activities (CPIA): 15%
- Resource Use/Cost Reporting: (based on claims data and calculated by CMS): 0% for 2017 (10% for following years)
Two terms you should be familiar with:
- Performance year: The year in which your practice performance is captured, measured and scored.
- Payment year: The year in which your performance year MIPS score is applied to your payments.
There is a two-year lag period between the performance year and the payment year. The first performance year is 2017, for which a bonus incentive or penalty will be applied to all federal payments in 2019, the payment year. (For more on this, see December’s “Coding Strategies” column, “The View Ahead…”)
The first performance year began on Jan. 1 and closes on Dec. 31. You must submit your data by March 31, 2018. If you didn’t begin reporting on Jan. 1, then you can begin anytime between Jan. 1 and Oct. 2, however the due date is the same.
HOW MUCH DO I HAVE TO REPORT?
The CMS site is explicit in 2017 provider options:
Do not participate: “If you don’t send in any 2017 data, then you receive a negative 4% payment adjustment.
“Test: If you submit a minimum amount of 2017 data to Medicare (for example, one quality measure or one improvement activity for any point in 2017), you can avoid a downward payment adjustment.
“Partial: If you submit 90 days of 2017 data to Medicare, you may earn a neutral or positive payment adjustment and may even earn the max adjustment.
“Full: If you submit a full year of 2017 data to Medicare, you may earn a positive payment adjustment.”
CMS also notes that you will not automatically be penalized for 90-day reporting if you missed the window for full-year reporting.
DO I REPORT AS AN INDIVIDUAL OR GROUP?
An individual is defined by CMS as a single clinician, with a single NPI, tied to a single Tax Identification Number (TIN). A group is defined by CMS as a set of two or more clinicians with unique NPIs, but sharing a common TIN.
Individual and group reporting have significant implications that should be understood:
- If you report as an individual, your payment adjustment (up, down or neutral) will be based on your individual performance.
- If you report with a group, each clinician will receive a payment adjustment (either up or down) based upon the group score.
- Individuals submit data through their EHR, or a registry, such as the AOA MORE system.
- When reporting with a group, submit data through the QPP website, your EHR, a registry or CMS beneficiary sample reporting. If using beneficiary sampling, you must register your group on the CMS Web interface by June 30. (For more on these options, visit qpp.cms.gov/learn/getprepared .)
WHAT DO I REPORT?
Each of the four categories, with three applicable for 2017, require unique information.
Quality: You will need up to six quality measures, including one outcome measure. For example, pick four or more of the following:
- POAG: optic nerve evaluation
- AMD: dilated macular exam
- AREDS: council for vitamins
- DM: dilated eye exam
- DR: communicate with PCP
- Tobacco screening
And then pick 1 or more of these (what we used to refer to as cross-cutting measures in PQRS):
- Document medications: dose, frequency, route.
- Measure BMI: height and weight.
- Close the referral loop: referral reports.
You can get extra credit, if you report more than six, as long as one is a cross-cut and one is an outcome measure. For example:
- Glaucoma: 15% reduction in IOP (Reduce IOP by 15% or have a plan to.)
- BP control: measure and advise plan if high
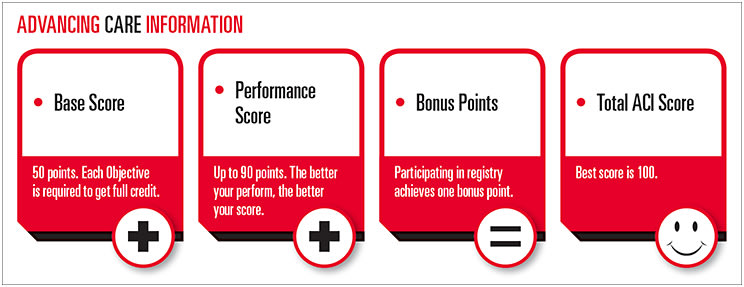
Advancing Care Information: In this area, participate in six base score categories by listing your numerator and denominator values.
The base categories are:
- Protect health information.
- Perform security risk analysis.
- E-prescribing
- Patient electronic access
- Provide access to portal.
- Provide patient specific education.
- Coordination of care
- View, download, transmit
- Secure messaging
- Patient-generated health data
- Health information exchange
- Exchange information with physicians.
- Exchange information with patients.
- Clinical information reconciliation.
- Clinical data registry (a listed measure, but most likely not applicable to optometry)
Of note, performance of these categories is not weighted to qualify for your base score. Performing each measure gets you the full base score of 50 points. Failing even one base score measure will result in a 0 score for ACI.
For your ACI performance score, each of the measures, grouped within the six categories, will be evaluated on how often you perform them. There are nine performance measures available and 90 total points for the section. Each performance measure is worth 10 points. Depending on the percentage of time performed, you will get a fractional score to apply.
For scoring purposes, in the Advancing Care Information performance category (weighted at 25% of the total CPS score), MIPS-eligible clinicians may earn a maximum score of up to 155%, but any score above 100% will be capped at 100%, according to the quality website. This structure was deliberately created to ensure that clinicians have flexibility to focus on measures that are the most relevant to them and their practices. (The best way to think about this is described by the graphic calculation on p.20.)
Clinical Practice Improvement Activities: This is a new category that comprises 15% of your total CPS score. These activities are designed for physicians to demonstrate how active they are in public health initiatives.
How you score this category depends on how you report, as an individual or as a group, and if a group, the number of CMS-qualified health care providers within the practice. The cutoff between a small and large practice is 15 health care providers. Groups with fewer than 15 participants, or if you are in a rural or health professional shortage area, would fall into the category of “small;” greater than 15 then you would fall into the “large” category.
The maximum score for CPIA is 40 points, for all reporting types. Using a registry helps greatly in this category.
According to the CMS QPP website, there are a total of 92 different measures. Here is a breakdown of the CPIA listings that could be applicable in optometry: (It is not a comprehensive listing.)
- Use registry to show practice patterns (20 points), for example, to learn how you treat and manage patients.
- Use registry to compare specific outcomes (10 points), for example, to compare your data vs. aggregate data for glaucoma.
- Use registry to show standards of practice care (10 points), for example, to compare your data vs. aggregate data.
- Use registry to promote adherence to treatment plans (10 points).
- Allow 24/7 access to clinicians (20 points).
- Collect patient experience and satisfaction data (10 points).
- Provide medication reconciliation with transition of care (10 points).
- Close referral loop: reports to referred physicians (10 points).
Resource Use/Cost Reporting: While not an area of active reporting for the 2017 performance year — as CMS will use actual claim data to calculate costs to the system — this will be a reportable area in years to come. Resource use can be thought of as a basis of how CMS will evaluate how cost effective you are in the system. Coordination of costs with specific ICD-10 codes will provide CMS with indications of costs associated with diagnoses and outcomes.
WHO WILL HAVE ACCESS TO THIS INFORMATION?
Understanding the importance of being visible in this new payment system is often understated. MIPS will publish each eligible clinician’s annual CPS and scores for each MIPS performance category within a year following the relevant performance year.
For the first time, consumers will be able to see their providers rated on a scale of 0 to 100 and how their providers compare to peers nationally. This level of transparency and specificity goes beyond prior programs, such as the Value-Based Modifier, which calculates quality and resource use scores, but did not publicly publish the results. Other third-party carriers will also have the ability to see your performance data and could use it in their decision-making processes, such as who will be invited to panel participation.
AM I TOO LATE FOR 2017?
Many of you may throw up your hands and say, “It’s too late.” But, it’s not! There are some very simple things that you can do to avoid a negative adjustment to your reimbursement, and possibly even qualify for a positive adjustment. Here are your three remaining options 2017.
- Don’t participate: Receive a negative 4% payment adjustment.
- Submit something: Submit a minimum amount of 2017 data (for example, one quality measure or one improvement activity for any point in 2017), to avoid a downward payment adjustment.
- Submit a partial year: Submit 90 days of 2017 data to earn a neutral or small positive payment adjustment.
Don’t let this new payment system create the age-old problem of over analysis, leading to paralysis. Work with your EHR vendor, and sign up with a registry to make this process easier on you and beneficial to your practice in the future.
When marketing itself to other health care stakeholders, optometry has often touted its ability to provide much more cost-effective care, greater population coverage, clinical skills and access than other professions.
This is the time to demonstrate your efficiencies and effectiveness as a healthcare provider to the system, so strive for the highest score you can get. Let’s demonstrate why we are clearly the primary eye care profession! OM
