


NEW TREATMENTS FOR NON-NEOVASCULAR (DRY) AMD MAY SOON BE AVAILABLE
IN “STAR WARS: EPISODE IV - A NEW HOPE,” we are introduced to the Death Star, a powerful moon-sized weapon that can obliterate a planet. It can be argued that AMD is like the Death Star: It too develops through different stages (as seen with the Death Star in the prequel “Rogue One: A Star Wars Story”) until it can destroy one’s vision, sometimes at laser speed.
Here, I discuss AMD, how to classify it and potential new treatments for dry AMD.
AMD
AMD is a progressive disease characterized by degenerative changes in the retinal pigment epithelium (RPE), Bruch’s membrane, the choriocapillaris and choroid, as well as the overlying photoreceptor layer. The condition is divided into early, intermediate and advanced.
Early disease is characterized by deposition of drusen, deposits comprised of lipids and inflammatory components, under the RPE cells into Bruch’s membrane. Intermediate disease reveals large drusen as well as hyper- or hypopigmentary changes in the RPE. The presence of large, soft confluent drusen is a significant risk factor for developing advanced AMD, which is divided into two camps: dry, or non-neovascular, and wet, or neovascular.
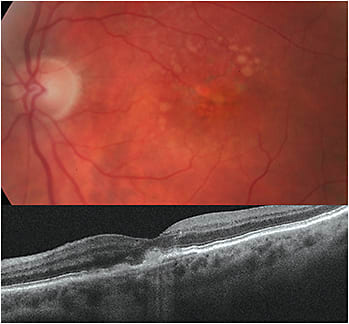
In dry AMD, geographic atrophy (GA) occurs. Sharply demarcated areas of RPE and choriocapillaris loss with appearance of underlying choroidal vessels in the macula characterize GA. Macular drusen generally fades in areas where GA develops. GA can initially cause visual disturbances, such as paracentral scotomas, which can impair vision in dim light, diminish contrast sensitivity and limit reading ability. As the disease progresses, it can result in devastating irreversible vision loss. The rate of progression is variable. The NIH-funded Age-Related Eye Disease Study (AREDS) shows progression from Intermediate AMD to GA takes approximately 2.5 to 5 years. About 85% to 90% of AMD cases are dry, reveals the American Macular Degeneration Foundation.
Wet AMD is characterized by the abnormal growth of blood vessels beneath the retina and choroidal neovascularization (CNV), stimulated by the protein vascular endothelial growth factor (VEGF). This can result in inflammation and damage to the macula, as these vessels can leak fluid and blood. The outcome: more rapid and more severe vision loss vs. dry AMD. A total of 10% to 15% of AMD cases are wet.
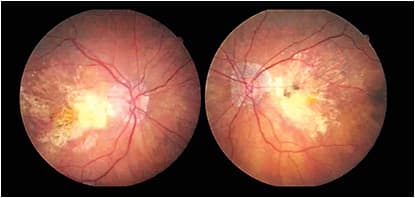
Dry and wet AMD are not mutually exclusive of each other and are likely to be bilateral. In fact, progression to the fellow eye ranges from 35% to 50% at five years, according to AREDS.
Risk factors for AMD include advanced age (50 and older), race (it’s more common in Caucasians), genetics (family history), systemic diseases, such as hypertension and hypercholesterolemia, and environmental influences, such as diet (high-fat), obesity, smoking and blue and ultraviolet light exposure. (Smoking cessation should be strongly recommended, as smoking significantly increases the risk of AMD progression.) All these factors contribute to the pathological process of drusen formation, lipoprotein deposition, oxidative damage, accumulation of lipofuscin, impaired choroidal perfusion and chronic inflammation in the macula. .
| DRY AMD | H35.3111 (Nonexudative AMD, OD, early stage) H35.3112 (Nonexudative AMD, OD, intermediate stage) H35.3133 (Nonexudative AMD, OU, advanced atrophic sans subfoveal involvement) H35.3134 (Nonexudative AMD, OU, advanced atrophic w/subfoveal involvement |
| WET AMD | H35.3211 (Exudative AMD, OD, w/active CNV) H35.3222 (Exudative AMD, OS, w/inactive CNV) H35.3233 (Exudative AMD, OU, w/inactive CNV) |
CLASSIFYING AMD
To determine AMD type, use the following:
- Amsler grid. This is essential in detecting metamorphopsia, central scotomas or micropsia that may indicate the presence of a CNV. Self-monitoring is important to alert AMD patients of any changes in vision.
- Dark adaptation. This device measures dark adaptation time and has been found to aid in the identification of early functional loss in AMD patients and those at risk for AMD, yet who have no clinical signs.
- Fluorescein and indocyanine green angiography. These detect the presence or recurrence, type, size and location of CNV, as well as determine the cause of vision loss not explained by the aforementioned test.
- Fundus autofluorescence (FAF). This detects RPE loss or dysfunction and enables you to track metabolic buildup of lipofuscin within the RPE. FAF can detect progression of GA or development of a CNV.
- Fundus photography. This is important for grading and staging AMD by capturing drusen, RPE abnormalities and atrophic lesions of GA or the presence of fluid or hemorrhage indicating a CNV. It enables the documentation of changes through time. It is worth noting that microperimetry can be used to reveal the amount of light recognized in specific parts of the retina.
- Macular Pigment Optical Density (MPOD). This is a measurement of the macular pigments, lutein and zeaxanthin, which help protect the photoreceptors from oxidative stress caused by absorption damage of ultraviolet and blue light. Low MPOD values have been associated with potential progression of AMD. Serial measurements let you monitor dietary changes and supplementation effects.
- OCT angiography (OCTA). This device allows for the visualization of the CNV vascular network. In addition, enhanced-depth imaging (EDI) provides improved visualization of the choroid, which allows for the assessment of choroidal changes in AMD.
- SD-OCT. This allows for the quantitative assessment of drusen, atrophic lesions and the detection of CNV changes, such as retinal fluid (intra/subretinal/sub-RPE), and response to therapy. Also, it reveals patchy thinning of the choriocapillaris in early dry AMD or loss of the RPE hyper-reflective structures with variable involvement of the overlying neurosensory retina, loss of the choriocapillaris and enhancement of the underlying choroid observed with GA.
POTENTIAL TREATMENTS
The NIH-funded AREDS studies reveal that supplementation containing vitamin C, vitamin E, lutein, zeaxanthin and zinc slow the progression of intermediate to late (dry and wet) AMD.
In addition, anti-VEGF therapy is effective in slowing or stopping the progression of wet AMD and, in turn, preserving vision. Further, a recent study on the use of two of these drugs through five years shows that almost half of the wet AMD patients who used the drugs had 20/40 vision or better, confirming the long-term benefits of the therapy, reveals Ophthalmology.
No effective treatments are available for dry AMD, but several clinical trials are focused on GA. Specifically, GA has been associated with the presence of inflammatory cells, such as macrophages, giant cells and mast cells within the retina and choroid, reveals the British Journal of Ophthalmology. Researchers have also found that drusen contains inflammatory proteins, including complement pathway activators. Thus, studies are underway to assess therapeutic complement inhibitors for GA.
The Phase 2 study, MAHALO, shows that the intravitreal administration of lampalizumab (Genentech, Inc.), a monoclonal antibody fragment designed to inhibit complement factor D, a rate-limiting enzyme of the alternative complement pathway implicated in the development of AMD, including GA, was able to reduce progression of GA.
As this article goes to press, Genentech has completed enrollment in two large Phase 3 clinical trials, Chroma (NCT02247479) and Spectri (NCT02247531), investigating the efficacy and safety of lampalizumab in reducing the progression of GA lesions secondary to AMD.
Finally, a recently published clinical trial reveals that some patients taking high doses of atorvastatin (Lipitor, Pfizer) experienced a complete resolution of lipid deposits in dry AMD. Investigators say they plan to further investigate the efficacy of a statin in a larger sample of dry AMD patients.
THE FORCE IS WITH US
(Spoiler alert!) At the end of “Star Wars: Episode IV – A New Hope,” the behemoth Death Star is destroyed. Although, we have not yet had the same success with dry AMD, among other sight-stealing eye diseases, we’re getting closer every day, as seen in the multitude of studies on possible forthcoming drugs. Staying abreast of and discussing these studies with your patients not only shows that you’re up to date on the latest information, but that you genuinely care about their ocular health. OM
